



Spine conditions
- Show All
-
Back health
-
lower back pain
-
Treatments
-
Lumbar Spinal Stenosis
-
sciatica
-
Spine conditions
-
Lumbar Pain
-
spinal stenosis

What is Spondylolisthesis? Causes, Symptoms, and Treatments
Spondylolisthesis is a spinal condition in which a vertebra (one of the bones that form the spi...

When to See a Doctor for Types of Severe Back Pain
Back pain slows down millions of Americans each year, with symptoms ranging from nuisance soren...

Spinal Surgery for a Slipped Disc
Each year, for every 1,000 adults, there are approximately 5 to 20 cases of disc herniation. Al...

Caring for Your Spinal Surgery Incision
All patients undergoing back surgery should actively ensure that the healing process goes a...

What Causes Back Pain?
Ancient medical experts believed that back pain was brought on by a fluid imbalance. Theref...

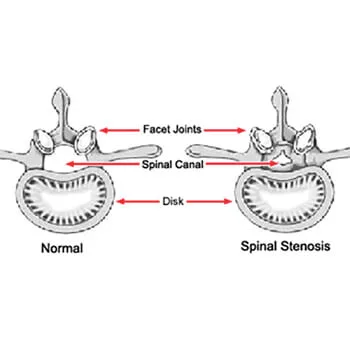
What is Lumbar Spinal Stenosis?
Spinal stenosis is a prevalent spinal disorder in the U.S. and across the globe. In fact, the c...

Is There a Cure for Lower Back Pain?
Lower back pain is among the most common medical problems affecting the human population. O...

What is a Lumbar Laminectomy?
Medical terminology doesn’t go out of its way to be complicated or hard to understand. It’s...

How Scoliosis Affects Life for Elderly People
Scoliosis is prevalent among children and teenagers. However, it can also have a large, far-rea...

What is Spondylolysis?
Although it’s not as common as spinal stenosis or a herniated disc, spondylolysis is near the ...

What is Laminoplasty?
Spinal stenosis is a prevalent spinal condition that can cause neck or back pain and neurologi...

What is Interspinous Process Fusion?
As we noted in our last blog, X-Stop, an implant deployed in the surgical treatment of mild sp...

Can You Get Blood Clots From Spinal Surgery?
Spinal surgery has made significant advances in both its safety and efficiency in correctin...

How much physical therapy do I need after spinal surgery?
Whether a patient is having open back surgery for a spinal cord injury or a minimally invasive...

Are some spinal surgeries more successful than others?
Are some spinal surgeries more successful than others? The short answer is yes, but that ...

Can Acupuncture Relieve Back Pain?
Not all advances in treating spinal disorders are necessarily new. Acupuncture has been practi...

What is Degenerative Joint Disease?
Osteoarthritis, commonly referred to as Degenerative joint disease, is a problem that often aff...

Causes of Back Pain in Adolescents vs. Adults
Though the majority of spinal problems appear between the ages of 35 and 55, wrought by nat...

Why are some spinal surgeons more successful than others?
It’s a fact that some spine surgeonshave higher success rates for the operations they per...

Choosing a Spinal Surgeon
Choosing a spinal surgeon is among the most important medical decisions a patient can make. A ...

Advantages of Medical Tourism
Can you really travel to a foreign destination for a vacation and receive high-quality medical...
How soon can you return to athletics after spinal surgery?
Near the top of the list of questions from almost every spinal surgery, the patients indica...

Taking Vitamins Before Surgery
Spinal surgery is stressful on the body. Anyone who is having spine surgery needs to prepare h...

Should I stop taking medications before spinal surgery?
You have a pinched nerve, slipped disc, a spinal cord injury, or other back problem that ...

What should I expect the day of my spinal surgery?
This is the big day, the day your spinal surgery will be performed and your back condition – b...

Post Op Day 1
You had your back surgery operation yesterday. The day after a lumbar laminectomy, spinal...

Recognizing and Preventing Post-Surgical Complications
With advanced procedures performed by highly trained and experienced surgeons, spinal surgery t...

What is Claudication?
Its name sounds complex, but the condition is very basic: Claudication is a pain, typically in...

Post Op Day 2
You had spinal surgery two days ago – perhaps it was for a simple but persistent pinched ...

What is Neural Claudication?
Recently, we addressed the topic of claudication. Claudication refers to pain typically felt in...

Having a Pinched Nerve in Your Lower Back
Your lower back is more susceptible to injury than the other regions of the spine. So, it’s uns...

What is Radiculopathy?
Have you heard of radiculopathy? This condition results from nerve irritation and, if it progre...

What is Lumbar Radiculopathy?
The human body contains an extensive system of nerves that facilitate communication between th...
What is Lumbar Spinal Decompression?
Lower back pain has long been a prevalent health concern around the world. In 2017, the preval...

Back Treatment Options
In our previous blog we discussed the tremendous stresses borne by the lumbar, or lower portio...

Sleep Tips for Back Pain Sufferers
Sleep provides important healing and rejuvenation to your back. When you’re suffering fro...

What is Failed Back Surgery Syndrome?
Failed back surgery syndrome (also called FBSS, or failed back syndrome) is a generalized t...