



What Is a Spinal Fusion? Overview, Types, & Recovery Timeline
Spinal fusion is a type of spinal surgery that permanently joins two or more vertebrae (the bones that form the spine) into a single bone. This eliminates all motion at the affected spinal level, helping to reduce the pain, instability, or nerve compression associated with conditions like spinal stenosis, spondylolisthesis, or herniated disc. Over 400,000 spinal fusion surgeries are performed each year in the U.S. (according to The Spine Journal), making it one of today’s most common spine procedures.
If you or a loved one is considering spinal fusion, you’re likely grappling with numerous questions: What exactly does the procedure entail? Am I a good candidate? How long will the recovery take? What are the risks? In this guide, we’ll answer all of these pressing queries and help you understand the best next steps toward pain relief.
Quick Answers: Spinal Fusion
- Recovery time: Return to office work at 1 to 3 months; 1 year for full recovery
- Success rate: 65 to 90%
- Alternatives: Endoscopic spinal decompression, motion-preserving implant, regenerative medicine
Spinal Fusion’s History, Prevalence, and Evolution
Spinal fusion has been performed since the 1900s, with Dr. Fritz Lange becoming one of the first to complete a spinal fusion surgery in 1909. Now, over 400,000 spinal fusion surgeries are performed each year in the U.S., according to The Spine Journal, making it one of the most common types of spine surgery. Since its inception, spinal fusion has evolved dramatically; in recent decades, minimally invasive approaches and motion-preserving solutions have paved the way for better outcomes and fewer complications.
To learn more about how spinal fusion has evolved with modern research, read our article: 10 Years After Spinal Fusion: Studies and Research.
How Does Spinal Fusion Work?
Spinal fusion works because bone graft material stimulates new bone growth and permanently fuses the affected vertebrae. This eliminates all motion at the spinal level, which may help reduce pain from spinal nerve impingement. Spinal decompression surgery, such as laminectomy, is often performed immediately before the fusion to reduce pressure on the compressed nerves.
During the spinal fusion, the surgeon accesses the spine through an incision, prepares the bone graft, secures the bone graft between the vertebrae, and closes the incision. These general steps can vary depending on the surgical approach.
The Role of Bone Grafts
Many bone graft options exist for spinal fusion, including local bone autografts, autografts, allografts, BMP, and synthetic bone. Autografts (bone taken from the patient’s own bone) are usually the preferred option because they contain living cells and compounds that support bone formation, and have a lower risk of rejection. While local bone autografts don’t require an extra incision, they may not provide sufficient bone quality or volume.
Autograft: The Gold Standard
An autograft is a bone graft taken from your own body. This type of bone graft is widely considered the gold standard for spinal fusion because, since it’s taken from the patient’s own body, it presents a lower risk of rejection than grafts from a foreign source. Autografts also contain growth factors and bone-forming cells (like osteoblasts, osteoclasts, and osteocytes) that support the fusion process.
For spinal fusion, autografts are generally taken from the iliac crest (hip bone). The downsides of an iliac crest autograft, according to a Journal of Spine Surgery study, include:
- An extra 30 to 40 minutes spent in surgery
- A second incision at the harvest site
- A potentially longer hospital stay
- Donor site morbidity (adverse effects at the iliac crest)
Local Bone Autograft
A local bone autograft utilizes the portions of spinal bone removed during spinal fusion surgery, repurposing it to help fuse the vertebrae. It uses the patient’s own bone and doesn’t require a separate incision. But, in some cases, there isn’t sufficient bone in this area for a successful fusion.
Some studies have found that local bone autografts may provide comparable outcomes to iliac crest autografts:
- A 2020 Global Spine Journal study found that there were no outcome differences between patients with low-grade spondylolisthesis who underwent TLIF (transforaminal lumbar interbody fusion) with either local autograft or iliac crest bone graft.
- Another Global Spine Journal study, published in 2015, found that a local bone graft is as safe and effective as an iliac crest bone graft for instrumented lumbar fusion to treat degenerative spine disease.
Allograft
An allograft is a bone graft taken from a donor. After being removed from the donor, an allograft is typically stored in a bone bank, where it’s sterilized and tested for various diseases. The hospital purchases the graft from the bone bank in preparation for the procedure.
The main benefit of using an allograft is that the patient doesn’t have to donate the tissue, which shortens the length of the surgery and prevents post-op iliac crest pain. However, allografts don’t contain living cells to support bone growth, so they may not heal as effectively as autografts.
Synthetic Bone Morphogenetic Protein (BMP)
BMP is a type of protein the body naturally produces, and it stimulates bone growth. Synthetic BMP (particularly recombinant human bone morphogenetic protein-2, or rhBMP-2) is a bone graft option for spinal fusion. A 2022 Journal of Spine Surgery study found that rhBMP-2 produces fusion rates that are comparable to (or higher than) those produced by autologous bone graft.
According to a World Journal of Orthopedics study, one of the key benefits of using rhBMP-2 in spinal fusion is that it doesn’t involve the adverse effects involved in iliac crest bone grafts (such as pain, infection, and sacral fracture). However, rhBMP-2 presents the risk of other adverse effects, such as:
- Inflammation and swelling
- Ectopic bone formation
- Bone resorption
Synthetic Bone
Synthetic bone graft materials omit the need to harvest bone from the patient. However, synthetic bone grafts don’t contain cells, so they must be mixed with other bone products for an effective fusion. In some cases, synthetic material may be combined with a small amount of autograft to increase the amount of graft material available for the procedure.
According to an International Journal of Spine Surgery study, two studies evaluating the use of ceramic (a type of synthetic bone graft) alone in spinal fusion reported fusion rates ranging from 77.6% to 90%.
Hardware: Screws, Rods, and Cages
Hardware (also known as instrumentation) is used in spinal fusion to stabilize the spine while the bone graft heals. It may also be used to help correct spinal deformities or misalignments. Fusion hardware is usually made of titanium, but other possible materials include polymers like PEEK (polyetheretherketone) and stainless steel.
The most common types of hardware used in spinal fusion include:
- Pedicle screws are secured through the pedicles, the cylindrical pieces of bone that extend backward from either side of the vertebral body.
- Rods are used to connect the pedicle screws, preventing movement at the affected spinal level.
- Interbody cages are used to maintain space between the two vertebrae, helping to reduce nerve root compression; replace the intervertebral disc material; and secure the vertebrae in place while the graft heals.
- Metal plates, such as the anterior plates used in anterior cervical discectomy and fusion (ACDF), are used for stability around the fused segment.
What Conditions Does Spinal Fusion Treat?
Spinal fusion is typically used to treat degenerative spinal conditions, including:
- Spinal stenosis, the abnormal narrowing of the spinal canal due to thickened ligaments, degenerative disc disease, bone spurs, or spondylolisthesis
- Spondylolisthesis, spinal instability causing a vertebra to slip downward, out of its normal alignment in the spine
- Spinal deformities (either congenital or degenerative) including:
- Scoliosis, an abnormal sideways spinal curvature creating an “S” or “C” shape, affecting an estimated 2 to 3% of the U.S. population, according to the American Association of Neurological Surgeons
- Kyphosis, an abnormal forward spinal curvature, generally caused by osteoporosis, degenerative disc disease, poor posture, or congenital issues
Am I a Candidate for Spinal Fusion?
You may be a candidate for spinal fusion if you have chronic, severe back pain that hasn’t responded to several months of non-surgical treatment. Additionally, candidates for spinal fusion often have limited mobility due to back pain and neurological symptoms.
Conditions Spinal Fusion Can Treat
Candidates for spinal fusion may have one of the following spinal conditions:
- Spinal fusion
- Spondylolisthesis
- Degenerative disc disease
- Herniated disc
- Vertebral fracture
- Scoliosis
- Spinal tumor
Underlying Medical Conditions
Some patients are not considered candidates for spinal fusion due to a severe, underlying medical condition, or an infection. Additionally, patients with a disease that impacts multiple spinal levels may be advised against spinal fusion surgery due to the higher risk of lost mobility.
Age Considerations for Spinal Fusion
Spinal fusion can be performed on adults between the ages of 20 and 80, meaning age alone is rarely a disqualification for the procedure. However, elderly patients are more likely to have underlying conditions that present surgical risks (such as an increased risk of pneumonia and cardiac problems). On the other end of the spectrum, young adults who undergo fusion are more likely to develop noticeable symptoms of adjacent segment degeneration and require reoperation, simply because they’ll live longer after the surgery.
Your doctor will consider these factors and recommend treatments accordingly.
Types of Spinal Fusion Surgery: Surgical Approaches
PLIF, ALIF, TLIF, and XLIF/LLIF are the primary types of lumbar spinal fusion surgery.
Quick Overview: PLIF vs. ALIF vs. TLIF vs. XLIF/LLIF
| PLIF | ALIF | TLIF | XLIF/LLIF | |
| Stands for | Posterior lumbar interbody fusion | Anterior lumbar interbody fusion | Transforaminal lumbar interbody fusion | Extreme lateral interbody fusion/lateral lumbar interbody fusion |
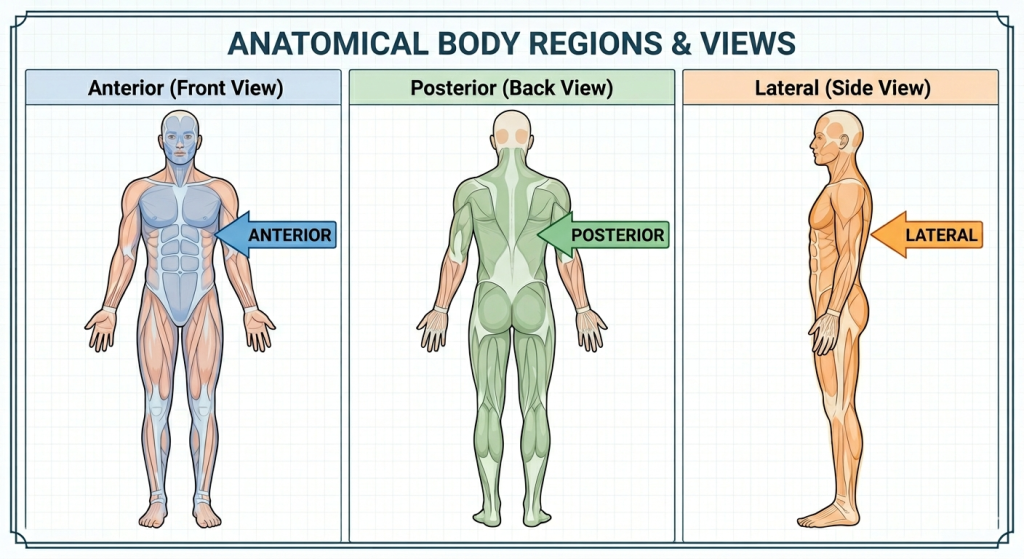
| Approach | Through the back | Through the front of the body | Through a midline back incision | Through the side/flank |
| Main benefit | Performed in a single stage; suitable for any spinal level | Avoids cutting through the back muscles | Facilitates minimally invasive techniques; lower risk to nerves | Minimally invasive; less muscle disruption and blood loss |
PLIF: Posterior Lumbar Interbody Fusion
PLIF involves accessing the spine posteriorly, or through the back. During this procedure, the surgeon will complete the following steps:
- First, the surgeon creates an incision in the back over the vertebrae to be fused. The back muscles must be moved aside to expose the spine.
- If applicable, spinal decompression is performed at this stage. This often involves removing part of the lamina, which covers the back of the vertebra.
- Once the decompression has been completed, damaged disc tissue is removed. The bone graft is placed in the disc space between the affected vertebrae. The graft is usually held in place with an implant, such as a spinal cage or interbody spacer.
- The back muscles are returned to their normal positions and the incision is closed.
ALIF: Anterior Lumbar Interbody Fusion
ALIF uses an anterior, or frontal, approach with the following steps:
- To start, the surgeon creates an incision in the lower portion of the abdomen and moves aside fat and muscle tissue to access the peritoneum. The peritoneum is a sack that contains the abdominal organs.
- Once the surgeon gains access to the peritoneum, they move it to the side to reach the spine without going through the abdomen. Large blood vessels are located over the front of the spine and must also be moved aside to perform the fusion.
- Decompression surgery may be performed at this stage.
- After removing the disc material, the surgeon positions the bone graft in the disc space with the help of an implant.
TLIF: Transforaminal Lumbar Interbody Fusion
Transforaminal lumbar interbody fusion is completed through the foramina, which are the bony openings located between adjacent vertebrae. This approach to spinal fusion may be suggested if the patient has spinal degeneration that’s mainly on one side of the spine.
- For TLIF, the surgeon creates an incision along the spine, directly above the affected vertebra. Similar to PLIF, the surgeon must move the back muscles aside to reach the spine.
- The surgeon can now access the disc space by drilling from one side of the spine, then extracting the lamina and/or facet joint.
- At this point, the damaged intervertebral disc material is removed and the bone graft is positioned in its place, secured by a fusion implant.
- The back muscles are repositioned and the incision is closed with sutures.
XLIF/LLIF: Extreme Lateral Interbody Fusion/Lateral Lumbar Interbody Fusion
XLIF is a minimally-invasive approach to spinal fusion. This is a relatively new surgical method that eliminates the need to create an incision in the abdomen or cut the large muscles of the back.
- First, the surgeon makes an incision in the flank, which is the lower back area of the abdomen. The peritoneum must then be moved away from the abdominal wall.
- Next, a dilator is placed into the peritoneum and moved toward the affected disc. The surgeon takes fluoroscopy images to confirm that the dilator is in the optimal position.
- To prevent nerve interference, a probe is placed through the psoas.
- At this stage, the surgeon removes the damaged disc and puts bone graft material in its place, through the incision in the flank.
- The peritoneum is returned to its usual position and the incision is closed with sutures.
Cervical Spinal Fusion (ACDF)
The most common approach for cervical (neck) spinal fusion is ACDF, anterior cervical discectomy and fusion. This procedure involves removing the damaged disc between two cervical vertebrae, then fusing them to treat nerve or spinal cord compression, usually from bulging discs, degenerative disc disease, bone spurs, or related conditions.
ACDF typically involves the following steps:
- The surgeon makes a (usually horizontal) incision on one side of the front of the neck. They must then move the trachea and esophagus to one side to access the cervical spine.
- Next, the surgeon removes the disc and, if necessary, other tissue (like bone spurs).
- In the open space left behind by the removed disc, the surgeon places bone graft material in between the vertebrae to stimulate fusion, along with any hardware to stabilize the area.
- After returning structures to their proper position, the surgeon closes the incision to complete the procedure.
Success rate: ACDF has a generally high success rate, with 88% of participants experiencing improvements or a full recovery following ACDF for degenerative disc disease in a 2023 BMC Musculoskeletal Disorders study.
How to Prepare for Spinal Fusion Surgery
To prepare for spinal fusion, you’ll need to undergo a thorough medical exam, implement healthy lifestyle habits, and prepare your home for the recovery period.
- Your pre-fusion medical exam may include:
- Radiograph assessment to evaluate alignment, stability, and degenerative changes
- Electromyography (EMG) for nerve function
- Imaging tests (MRI) to evaluate nerve impingement
- General physical exam to ensure you’re healthy enough to undergo surgery
- The most crucial lifestyle adjustments to implement before spinal surgery include:
- Quitting smoking (smoking has been linked to lower fusion success rates and higher complication rates, according to the International Journal of Spine Surgery)
- Reaching a healthy weight and prioritizing physical fitness
- Stop drinking alcohol at least 48 hours before surgery
- Stop taking anti-inflammatory medications (aspirin and other NSAIDs, like ibuprofen) at least seven to 10 days before surgery
- To prepare your home for a smooth recovery period:
- Meal prep or consider DIY meal kits
- Stock your freezer with ice packs and purchase a heating pad
- Place essential items within reach to prevent bending, twisting, and reaching
- Complete basic chores, like laundry and cleaning
- Prepare the bathroom with a shower seat or mat and toilet riser
- Arrange to have help around the house (from a loved one or caregiver) in the first two weeks after surgery
Also, make sure to talk to your doctor for personalized recommendations as you prepare for spinal surgery.
Spinal Fusion Recovery Timeline
Spinal fusion recovery is a relatively long process involving several stages. Your surgeon will help guide you through these stages, advising you on the activities that you can resume – and those that you should continue to avoid.
Here’s a general timeline of the spinal fusion recovery process, from the hospital stay to a full recovery:
Hospital Stay: 2 to 4 Days
Spinal fusion usually requires a hospital stay of two to four days. Minimally invasive procedures may allow for a shorter hospital stay, while more invasive approaches require a longer stay. Your stay will involve:
- Pain management with medications such as acetaminophen, NSAIDs, muscle relaxants, or IV opioids (for the short-term)
- Early-stage mobility work with a physical or occupational therapist: You’ll learn how to safely complete basic, essential tasks, like getting out of bed, sitting, standing, walking, and getting dressed.
- Incision care to ensure your incision remains dry and clean
- Back bracing (in some cases) to prevent excessive spinal motion

Your post-op progress will be monitored throughout your hospital stay, and you may be cleared to return home if your pain is effectively managed (with oral medications) and you’re able to get out of bed unassisted, with no indications of infection.
1 to 4 Weeks
Overview: Pain medication, assistance around the house, possible return to sedentary work
During this phase of your recovery, your activities will be relatively limited. You may still need help to complete light housework, and you’ll likely still need medication for pain management.
However, if you have a sedentary job, you may be able to return to work within a few weeks of the procedure. You’ll need to avoid bending or twisting the spine, lifting anything other than light objects, and driving.
1 to 3 Months
Overview: Return to basic housework and low-intensity work, potential return to driving, physical therapy
One to three months after spinal fusion, you’ll start to complete basic chores around the house. Your doctor may also clear you to drive during this stage. However, you still won’t be able to bend, twist, or lift heavy objects.
During this phase, you’ll be attending physical therapy to ensure that the spine heals properly. A physical therapist will help you regain strength and mobility without jeopardizing the fusion process.
3 to 6 Months
Overview: Return to low-intensity cardio, fewer restrictions
During this stage of spinal fusion recovery, you can gradually return to cardiovascular exercise and stretching. While you won’t be able to bend the spine or lift heavy objects, your activities won’t be as restricted.
6 Months to 1 Year
Overview: Success determination, complete recovery
During this period, your surgeon can determine if the fusion was successful. If the vertebrae fused properly and the spine appears healthy, you can return to most of your usual activities, including bending and twisting the spine. Keep in mind that some mobility is lost to the fusion process, so your spinal mobility will still be somewhat limited.
Beyond the 1-year mark, your vertebrae may continue to heal, along with any damaged nerves. In some cases, spinal nerve damage takes two years to heal completely. However, most patients are virtually pain-free after a year of recovering from spinal fusion.
Risks and Complications of Spinal Fusion
The risks and complications of spinal fusion include limited mobility, pseudoarthrosis, adjacent segment disease, recurrent pain, and muscle atrophy. These risks are in addition to those of all surgical procedures, such as infection, blood clots, and adverse reactions to anesthesia.
Limited Mobility
Limited mobility can occur after spinal fusion due to lost mobility at the fused segment. Once the vertebrae have fused into a single bone, the patient loses the ability to bend or twist at that segment. In some cases, patients require a reacher tool to retrieve items on the floor after spinal fusion.
Lost mobility is particularly common after multi-level fusions. However, even for patients undergoing a single-level fusion, it’s crucial to talk to your surgeon about how lost spinal mobility could impact your lifestyle.
Pseudoarthrosis
Pseudoarthrosis, or failed fusion, occurs when the vertebrae fail to fuse after the surgery. Unfortunately, pseudoarthrosis continues to be a risk with modern fusion methods. This complication typically creates the need for additional surgery.
According to a clinical review published in 2022, rates of pseudoarthrosis range greatly from 0% to 20% to greater than 60%, depending on which study you reference. A 2015 study noted that at least 15% of patients who undergo primary lumbar fusion experience pseudoarthrosis.
While the exact rate of pseudoarthrosis is unclear, it’s a distinct risk, particularly for patients who smoke, use steroids or have diabetes.
Adjacent Segment Disease
Adjacent segment disease, or ASD, is a possible complication of spinal fusion. It develops when the spinal segments above and below the fused segment degenerate more rapidly than usual. This occurs because the adjacent segments must compensate for the lost motion at the fused segment.
As the adjacent segments start to degenerate, patients may experience back pain and/or neurological symptoms, such as tingling, weakness, and numbness. Eventually, some patients with ASD require reoperation to resolve their symptoms.
ASD is estimated to impact 11 to 12% of patients 5 years postoperatively and 16 to 38% at the 10-year mark.
Recurrent Pain
In some cases, spinal fusion surgery doesn’t resolve the patient’s back pain. This may occur in up to 40% of patients.
Muscle Atrophy
Muscle atrophy is the term used for muscle tissue that thins out or wastes away. Since spinal fusion limits how much patients can use their back muscles, it can lead to muscle atrophy. When the muscle tissue around the spine atrophies, it reduces support for the spine and increases the risk of future injury.
Surgical Risks
All surgical procedures come with certain risks, including:
- Hemorrhage
- Shock
- Deep vein thrombosis
- Pulmonary embolism
- Infection
- Allergic reactions to anesthesia
To further explore the possible risks of undergoing spine surgery, read our blog article: What Are The Risks of Back Surgery?
Alternatives to Spinal Fusion
Given the risks and complications of spinal fusion, many patients look for alternative treatment options. Thankfully, the latest advancements in medical technology have paved the way for fusion alternatives, including the TOPS System.

David danced at his son’s wedding Bonnie explains why TOPS surgery was the right decision for her Wade is back to hiking Scott speaks about going to surgeryTake back control of your life with Premia Spine!




Regain your mobility with Premia Spine! Contact us now
The TOPS System is an FDA-approved non-fusion implant that stabilizes the spine without permanently fusing the vertebrae or compromising the patient’s range of motion. It moves with the spine, preventing lost mobility, adjacent segment disease, and related complications. It has earned a superior-to-fusion claim from the FDA, making it one of the most compelling fusion options available today for lumbar spinal stenosis and degenerative spondylolisthesis.
Other fusion alternatives include:
- Conservative methods like physical therapy, lifestyle adjustments, pain medications, steroid injections, massage therapy, and acupuncture (may not be sufficient in cases of advanced spinal degeneration)
- Endoscopic spinal decompression, a minimally invasive approach to spinal decompression surgery that uses a tiny camera to drastically reduce incision size and tissue damage
- Regenerative medicine, such as stem cell therapy, an emerging treatment option that involves using regenerative materials to stimulate tissue regeneration without invasive methods
Talk to a spine specialist in your area to learn more about alternatives to fusion for chronic spinal conditions.
FAQs: Spinal Fusion
What is the success rate of spinal fusion?
Ranges from 65 to 90% based on patient age, overall health, and surgical approach
How much does spinal fusion cost?
Direct costs for single-level lumbar fusion range from $8,286 to $73,727, according to the Global Spine Journal.
Can you live a normal life after spinal fusion?
Most patients return to a normal or near-normal life after spinal fusion, with some movement restrictions. One of the biggest threats to this is the risk of adjacent segment degeneration after fusion, which can lead to new or recurring back pain.
What can you never do again after spinal fusion?
Heavy weightlifting, contact sports, jumping on a trampoline, and deep or repetitive bending or twisting (from gymnastics, intensive yoga, etc.)
How long does it take to walk again after spinal fusion?
Up to a few days; you’ll work with an occupational therapist to regain the ability to walk safely before leaving the hospital.
How long do you have to stay in bed after spinal fusion surgery?
While bed rest is necessary for the first few days after spinal fusion, prolonged bed rest should be avoided to prevent stiffness and encourage blood flow to the fused segment.