



What is Spondylolisthesis? Causes, Symptoms, and Treatments
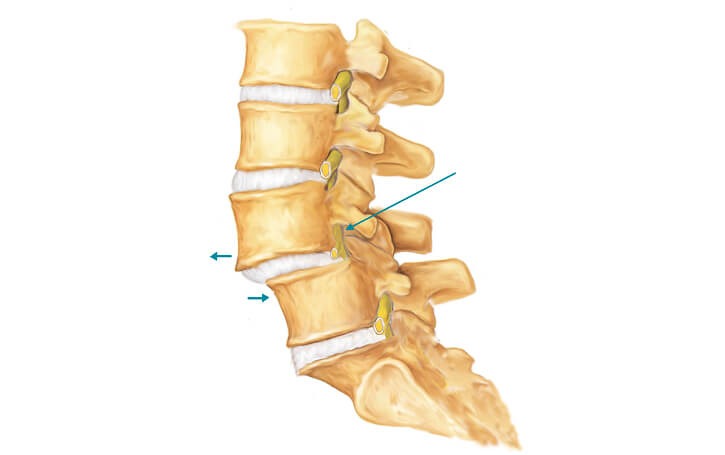
Spondylolisthesis is a spinal condition in which a vertebra (one of the bones that form the spinal column) slips forward over the vertebra beneath it, most often in the lower back (lumbar spine). The word comes from two ancient Greek words: “spondylos” (vertebra) and olisthesis (to slip or slide). It’s fairly common, with a prevalence rate of approximately 2.7% in men and 8.4% in women (for degenerative spondylolisthesis, according to StatPearls).
Below, we’ll discuss the most prevalent causes, typical symptoms, and available treatments for spondylolisthesis to help guide your recovery journey. For symptoms lasting longer than a few weeks or that become severe, contact your spine specialist for an evaluation.
Spondylolisthesis at a Glance:
- Causes: Age-related degeneration, stress fracture, spinal defects, genetic factors
- Symptoms: Lower back pain, stiffness, sciatica, tight hamstrings
- Treatments: Physical therapy, medications, surgery (for severe cases)
Spondylolysis vs. Spondylolisthesis: What’s the Difference?
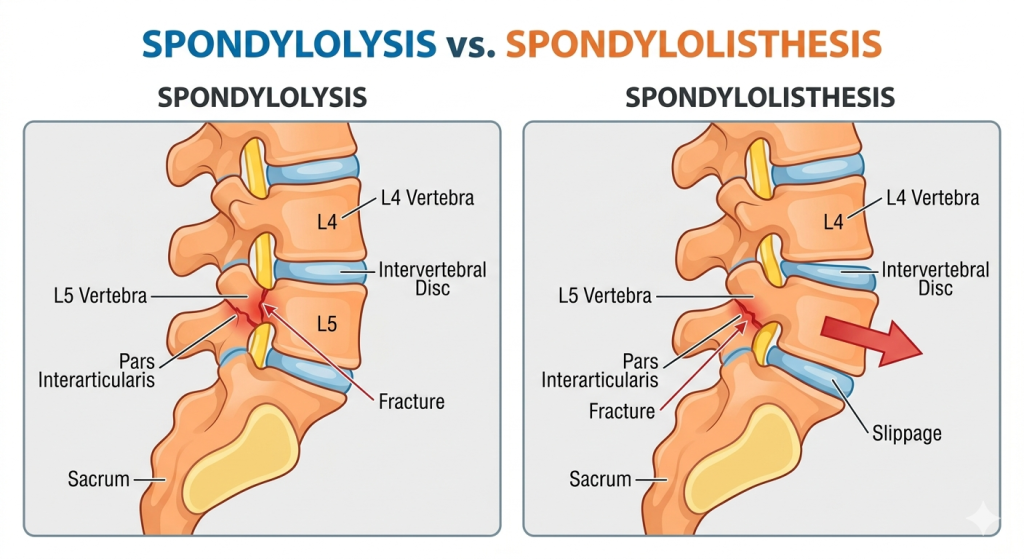
Spondylolysis is a stress fracture that runs through the pars interarticularis, a small segment of bone that connects two vertebrae. Spondylolisthesis is the downward slippage of a vertebra due to instability; spondylolysis is a possible cause of spondylolisthesis.
When the pars interarticularis is fractured, patients may experience back pain that worsens with physical activity. However, not all spondylolysis patients have symptoms.
Approximately one out of 20 people has spondylolysis, making it a relatively common condition. Additionally, spondylolysis can lead to spondylolisthesis. This is because the pars interarticularis fracture can diminish the stability of the spine and potentially lead to slippage.
What is Spondylosis?
Spondylosis refers to spinal degeneration, usually related to aging. Over time, it can lead to degenerative spondylolisthesis. Spondylosis is very common among older adults, with prevalence rates upwards of 95% by age 65.
Is Spondylolisthesis The Same As a Slipped Disc?
No, spondylolisthesis isn’t the same as a slipped disc. Spondylolisthesis involves a vertebra that slips out of position, while a slipped disc is an injured spinal disc. While the common medical term “a slipped disc” may seem to indicate the slippage involved in spondylolisthesis, it’s an entirely different condition.
Spondylolisthesis affects the spinal bones, which are known as vertebrae. A slipped disc is an injury involving an intervertebral disc, which is a cushion of shock-absorbing tissue. There’s an intervertebral disc located in between each of the vertebrae in the spine.
Types of Spondylolisthesis
Degenerative spondylolisthesis is the most common type, followed by isthmic spondylolisthesis. Other possible types include congenital, traumatic, and pathological.
- Degenerative spondylolisthesis: The most common cause of spondylolisthesis is degenerative changes in the vertebral joints and cartilage due to aging.
- Isthmic spondylolisthesis results from a defect in the pars interarticularis, potentially from:
- A stress fracture (spondylolysis), commonly from overuse in teen athletes
- Genetic factors, including naturally thinner pars interarticularis, and spinal anatomy
- Congenital spondylolisthesis (also known as dysplastic spondylolisthesis) is caused by a birth defect in the facet of the vertebra. The defect, which is present at birth, can cause the vertebra to slip out of position. This is referred to as dysplastic spondylolisthesis.
- Traumatic spondylolisthesis may be caused by:
- Spinal trauma: Spondylolisthesis can also result from sudden trauma, such as a sports injury or car accident. This is known as traumatic spondylolisthesis and can occur in people of all ages.
- Sports injury: In athletes who repetitively strain and overstretch the spine, spondylolisthesis is a relatively common injury. This is especially true in younger athletes, given that their spines haven’t fully developed.
- Pathological spondylolisthesis results from underlying conditions that compromise bone strength, like osteoporosis or a tumor.
Understanding Grades of Spondylolisthesis: The Meyerding Classification System
The Meyerding classification system defines five grades of spondylolisthesis, and it’s used to evaluate the condition’s severity based on a lateral spine X-ray image. It may be used to help clearly diagnose spondylolisthesis and help patients better understand the extent of the vertebral slippage.
To use this system, the medical professional draws a line through the posterior (back) wall of the superior and inferior vertebral bodies. They then calculate a percentage of the distance between the two lines to measure the movement of the vertebral body above.
The five grades of spondylolisthesis, according to the Meyerding system, are:
- Grade 1 spondylolisthesis is a 0 to 25% slippage.
- Grade 2 spondylolisthesis is a 26 to 50% slippage.
- Grade 3 spondylolisthesis is a 51 to 75% slippage.
- Grade 4 spondylolisthesis is a 76 to 100% slippage.
- Grade 5 spondylolisthesis, or spondyloptosis, is an over 100% slippage.
What Does Spondylolisthesis Feel Like?
Spondylolisthesis generally feels like persistent lower back pain and stiffness, potentially with nerve-related symptoms like sciatica, tingling, and numbness.
- Lower back pain: The most frequent symptom of lumbar spondylolisthesis is lower back pain. The pain typically worsens after exercise and abates when you sit or bend forward.
- Reduced mobility: Decreased range of motion and tightness of the hamstring muscles are common spondylolisthesis symptoms.
- Sciatica: Lumbar spondylolisthesis can cause sciatica, the term for compression of the sciatic nerve, which extends from the lower lumbar vertebrae into the buttocks and down the backs of the legs. Sciatica symptoms include:
- Burning, shooting, or electric shock-like pain down one or both legs
- Tingling, numbness, or pins and needles sensation
- Muscle weakness
- Muscle tightness, especially in the hamstring muscles
While not exactly a symptom of spondylolisthesis, spinal stenosis, an abnormal narrowing of the spinal canal, can be caused by degenerative spondylolisthesis.
Who’s at Risk for Spondylolisthesis?
Risk factors for spondylolisthesis include being over age 50, female, overweight, participating in high-impact activities, pre-existing medical conditions, and a family history of the condition.
Age: Over 50
Adults over age 50 are more vulnerable to degenerative spondylolisthesis due to age-related spinal changes and cumulative wear and tear. Age-related spinal changes that can contribute to spondylolisthesis include:
- Drier, weaker spinal discs
- Weakened spinal ligaments
- Arthritic facet joints (spondylosis)
Female Gender
Women are significantly more likely to develop degenerative spondylolisthesis: it affects an estimated 8.4% in women and 2.7% in men, according to StatPearls. This is likely due to a combination of factors, including:
- Menopause-related hormonal shifts (reduced estrogen)
- Anatomical differences
- Increased ligament laxity
Family History and Pre-Existing Conditions
A family history of spondylolisthesis, particularly from genetic spinal abnormalities like thinner pars interarticularis, increases your risk of developing the condition. Certain pre-existing conditions can also increase your risk, including spondylolysis, spondylosis, and osteoporosis.
Obesity
Increased body weight from obesity increases the mechanical load on the lumbar spine, which can exacerbate spinal wear and tear. This leaves the spine more vulnerable to degenerative conditions, including spondylolisthesis.
In a large-scale epidemiological study using the Medicare Claims 5% Limited Data Set, obese individuals had approximately 1.84 to 3.75 times the prevalence of most degenerative spinal conditions compared to non-obese individuals.
Sports and Physical Activities
Spondylolisthesis in athletes may occur, particularly in sports that involve a high degree of impact, deep spinal bends, twists, and extensions, and intense axial loading (heavy overhead lifting). Another prominent risk factor is in young athletes, who are more prone to spondylolysis (spinal stress fracture), which can destabilize the spine and lead to spondylolisthesis. Spondylolysis rates in teen athletes as high as 30% have been reported, according to the Journal of Sports Medicine.
Physical activities that may increase your risk of developing spondylolisthesis include:
- Contact sports
- Weightlifting and powerlifting
- Figure skating
- Dancing
- Tennis
- Baseball
- Diving
- Rowing
Warning Signs: When to See a Spine Specialist
It’s time to see a spine specialist for spondylolisthesis if you experience:
- Pain that lasts longer than two weeks or consistently worsens
- Sciatica
- Difficulty walking
Though rare, lumbar spondylolisthesis can cause cauda equina syndrome, a medical emergency involving compression of the cauda equina, a sack of nerve roots at the base of the spine. If you experience any of these warning signs of cauda equina syndrome, go to the ER immediately for emergency medical care:
- Saddle anesthesia (numbness or tingling in the inner thighs, groin, or buttocks)
- Severe, sudden, or rapidly progressing numbness or weakness in the legs
- Changes in bowel or bladder function
- Sudden sexual dysfunction
How is Spondylolisthesis Diagnosed?
A physician specializing in spinal disorders can diagnose spondylolisthesis using radiographs and X-ray imaging, as well as a comprehensive physical exam. You’ll likely stand sideways as the X-rays are taken so your physician can see the vertebra’s slippage clearly (this is called a standing lateral X-ray).

After your physician has examined the imaging test results, the severity of your spondylolisthesis case will be graded. The grading scale is based on the degree of slippage from the vertebra’s normal position, using the Meyerding classification system (as discussed above).
Upon making a diagnosis, a physician can recommend appropriate treatments for spondylolisthesis.
What Makes Spondylolisthesis Worse?
Several factors can worsen spondylolisthesis, including:
- High-intensity physical activities
- Heavy lifting
- Poor posture
- Being involved in an auto accident
If you’ve been diagnosed with spondylolisthesis, your physician likely recommended lifestyle adjustments to help you avoid the factors listed above.
Spondylolisthesis Exercises To Avoid
Any exercises that involve heavy lifting and excessive twisting or bending should be avoided with spondylolisthesis. If you enjoy a specific sport, you should talk to your physician about whether it’s safe to participate in that sport while you’re struggling with spondylolisthesis symptoms.
Sports that tend to exacerbate spondylolisthesis symptoms include:
- Weightlifting and powerlifting
- Running
- Football
- Soccer
- Diving
- Competitive swimming
- Gymnastics
- Certain types of dance, including ballet
Non-Surgical Spondylolisthesis Treatments
Non-surgical treatments for spondylolisthesis include physical therapy, exercises for relieving pressure on the affected spinal nerves, medication, and epidural steroid injections. In many patients, these treatments are sufficient to alleviate the symptoms of spondylolisthesis.
| Conservative Treatments for Spondylolisthesis | ||
| Treatment | Benefits | Best for |
| Physical therapy | Develops muscles that stabilize the spineImproved posture & body mechanicsSupports mobilityDrug-free | Low-grade spondylolisthesisPost-surgery |
| Chiropractic care | Improved spinal alignmentMay help calm nerve compressionDrug-free | Early stages of spondylolisthesisIn combination with other conservative methods |
| Medications | Helps relieve pain & other symptoms | Short-term symptom managementPost-surgery pain relief |
| Epidural steroid injections | Helps reduce inflammation & pain | Temporary pain relief |
What Does Physical Therapy For Spondylolisthesis Involve?
Physical therapists can help patients manage spondylolisthesis in several ways.
For one, your PT can offer valuable insights and education about how your lifestyle is affecting your symptoms. From your exercise regimen to your footwear to your posture, your physical therapist can identify areas for improvement. In making the recommended adjustments, you can likely reduce the pressure on your spine, leading to an improvement in spondylolisthesis symptoms.
Additionally, your PT can implement various non-invasive methods of pain management. Targeted heat and cold therapy can help alleviate inflammation and pain. Electrical stimulation is another popular method among physical therapists to gently reduce the transmission of pain signals to the brain.
Physical therapists can also recommend stretching and strengthening exercises for spondylolisthesis. By stretching to reduce muscle tension, you can gain greater back flexibility. By strengthening various muscle groups, you can gain greater stability in the lumbar spine, hips, and pelvis.
Does Chiropractic Care Help With Spondylolisthesis?
Many spondylolisthesis patients find that chiropractic care is a helpful tool for alleviating their symptoms; it’s particularly popular among those looking to treat spondylolisthesis naturally. Chiropractors specialize in spinal manipulation to treat issues involving the musculoskeletal system.
Key goals of chiropractic care for spondylolisthesis include improving spinal mechanics, restoring spinal function, and improving posture. In achieving these goals, your chiropractor may alleviate compression on the spinal nerves, which often leads to reduced symptoms.
One of the main benefits of chiropractic care for spondylolisthesis is that it’s non-invasive. Chiropractors focus on methods including manual and instrument-assisted manipulation to adjust the spine, making it a safe back pain treatment option.
Which Medications Are Used To Treat Spondylolisthesis?
Physicians often recommend over-the-counter medications to help spondylolisthesis patients manage pain and inflammation. In more advanced cases that don’t improve with over-the-counter options, physicians may instead suggest prescription medications.
There are a few different types of drugs that may help with spondylolisthesis. The main types include:
- Analgesics
In simpler terms, analgesics are painkillers. These over-the-counter medications’ primary function is to relieve pain. The most common analgesic is acetaminophen, or Tylenol.
- NSAIDs (non-steroidal anti-inflammatory drugs)
NSAIDs alleviate inflammation along with pain. There are numerous over-the-counter NSAIDs, such as aspirin, Aleve, and Advil (ibuprofen), as well as prescription NSAIDs.
- Neuropathic agents
This type of prescription medication can be helpful for patients suffering from spondylolisthesis nerve pain. Neuropathic agents target nerve pain directly and can help with spondylolisthesis symptoms, including tingling, numbness, and weakness.
Gabapentin and pregabalin (Lyrica) are two of the most commonly prescribed neuropathic agents for spondylolisthesis.
- Muscle relaxants
Some spondylolisthesis patients experience chronic back pain caused by muscle spasms in the back. In these cases, physicians may prescribe a muscle relaxant to stop the spasms. Soma, Flexeril, Baclofen, Tizanidine, and Robaxin are among the most widely prescribed muscle relaxants.
To learn more about conservative strategies for spondylolisthesis symptom management, check out our blog article: Spondylolisthesis Self-Care: Effective Pain Management Techniques for Daily Relief
Epidural Steroid Injections
Epidural steroid injections involve injecting steroid medication into the epidural space (the area surrounding the spinal cord). The treatment goal is to reduce inflammation around the spinal nerves to alleviate pain. However, pain relief from steroid injections is typically temporary, and it’s not recommended to receive them more than three times annually, as doing so may lead to complications like weakened muscles and reduced bone density.
Success Rate of Epidural Steroid Injections for Spondylolisthesis
A study in the Journal of Back and Musculoskeletal Rehabilitation reported epidural steroid injection success rates of 66.1% for degenerative spondylolisthesis and 46.9% for isthmic spondylolisthesis. However, a study in the Journal of Bone and Joint Surgery found that epidural steroid injections may help relieve pain from degenerative spondylolisthesis for up to four months, but had little effect on the eventual need for surgery.
Spondylolisthesis Surgery: Approaches and Fusion Alternatives
For patients with moderate to severe spondylolisthesis who don’t respond to conservative therapies, physicians may recommend spinal decompression surgery. The idea of undergoing surgery can be daunting, but note that most patients’ symptoms improve with non-surgical treatment.
If you and your physician determine that spondylolisthesis surgery is the right treatment route, you’ll likely discuss the spinal decompression procedure.
What is Spinal Decompression?
Spinal decompression involves removing portions of the vertebrae that impinge on the spinal cord and nerve roots. There are several different approaches to spinal decompression, including laminectomy, foraminotomy, discectomy, and corpectomy. For spondylolisthesis, surgeons often opt for a laminectomy.
Laminectomy involves removing some or all of the lamina. This is the small section of bone that covers the back of the spinal canal. By removing it, your surgeon can create more space for the spinal nerves and alleviate nerve impingement.
Spinal decompression can have a dramatic effect, relieving pain and other spondylolisthesis symptoms. However, removing portions of the lamina reduces the stability of the spinal column. So, after decompression surgery, spinal stability remains a key concern for spondylolisthesis patients.
This is why surgeons traditionally perform spinal fusion after spinal decompression.
What is Spinal Fusion?
Spinal fusion involves placing bone graft material in between the affected vertebrae. Then, screws and rods are implanted to secure the graft in place and provide additional stability.
In the period following spinal fusion surgery, the bone graft material will spur the permanent joining of the affected vertebrae. This prevents all movement between the fused vertebrae, which can prevent instability in spondylolisthesis patients.
Unfortunately, in stabilizing the vertebrae, spinal fusion eliminates the natural independent motion that gives the spine flexibility. This diminishes patients’ ability to carry out certain movements, namely those that require the bending or twisting of the spine. Fusion has also been shown to promote the deterioration of adjacent vertebrae.
The TOPS™ System For Spondylolisthesis

For those looking for motion-preserving fusion alternatives for spondylolisthesis, there’s the TOPS™ System. It’s a dynamic non-fusion that replaces the tissues removed during spinal decompression and establishes a controlled range of spinal motion. TOPS™ is FDA approved to treat degenerative spondylolisthesis (up to grade I) at one level from L3 to L5 with moderate to severe lumbar spinal stenosis, and it’s earned a superior-to-fusion claim from the FDA.
Regain your mobility with Premia Spine! Contact us now
David danced at his son’s wedding Bonnie explains why TOPS surgery was the right decision for her Wade is back to hiking Scott speaks about going to surgeryStart your recovery process Today!




In a seven-year study for patients with degenerative spondylolisthesis and lumbar spinal stenosis, the TOPS™ System maintained clinical improvement and stability. Additionally, in a five-year study of the TOPS™ System for 10 patients with degenerative spondylolisthesis and lumbar spinal stenosis, the clinical outcome scores “improved significantly across all scoring systems”. In this study, there were no failures at five years and no patients required revision surgery.
TOPS™ Testimonials
Patient and surgeon testimonials are highly encouraging for the TOPS™ System as a spondylolisthesis treatment. Many patients note that they’re able to return to their favorite activities after the TOPS™ procedure, as it preserves spinal mobility.
We encourage anyone with persistent back problems to consult a physician who specializes in spinal disorders and learn about the latest available treatment options.
FAQs: Spondylolisthesis
What’s the difference between spondylolysis and spondylolisthesis?
Spondylolysis is a fracture in the pars interarticularis; spondylolisthesis involves the slip of the vertebra that can result from spondylolysis.
What should I not do with spondylolisthesis?
Heavy lifting, high-impact activities, excessive spinal twisting or bending
How long to rest with spondylolisthesis?
Avoid staying in bed longer than one to two days; take a break from intense exercise, but engage in light, low-impact movement (like walking)
Can spondylolisthesis get worse over time?
Yes, spondylolisthesis can get worse over time if it’s left untreated.
Can spondylolisthesis be cured without surgery?
While the slip itself can’t be “cured” without surgery, spondylolisthesis is often successfully treated without surgery, especially if it’s addressed promptly.