



What Are The Symptoms of Severe Spinal Stenosis of The L4-L5 Segment and How to Treat It?
Severe spinal stenosis at L4-L5 is a debilitating condition that occurs when the spinal canal narrows and compresses the L4 and L5 nerve roots in the lower back, often due to age-related spinal degeneration, damaged discs, or thickened ligaments. Key symptoms include lower back pain, numbness, tingling, weakness, walking difficulties, and neurogenic claudication (spinal nerve compression symptoms that improve when you sit or lean forward). Severe symptoms of L4-L5 stenosis can escalate to serious mobility loss, foot drop, and bladder and bowel symptoms, which require prompt medical care.
In this article, we’ll explore the hallmark symptoms of severe spinal stenosis of the L4-L5 spinal segment, along with why they develop, how they’re diagnosed, and the treatment options available to you.
Understanding L4-L5 Anatomy: Why This Segment Is Vulnerable
The L4-L5 spinal segment consists of the two lowest vertebrae in the lumbar spine, the L4-L5 disc, two facet joints, and various muscles, ligaments, nerves, and bony processes.
Two key factors make this segment particularly vulnerable to spinal stenosis: Weight bearing and flexibility.
- L4-L5 bears significant weight to support the torso and upper body.
- L4-L5 is the most mobile spinal level and allows your torso to move in many directions, including:
- Flexion (forward bending)
- Extension (backward bending)
- Rotation
- Lateral (side) bending
Symptomatic L4-L5 stenosis often involves L4-L5 nerve root compression. The L4-L5 nerve roots are the lowest nerve roots of the lumbar spine and supply sensation to the thigh muscles, lower legs, outer legs, hamstring muscles, ankles, tops of the feet, between the toes, and certain pelvic organs (as part of the sacral plexus). The cauda equina (a collection of nerve roots located in the lumbar spine) is typically located between spinal levels L1 and L5.
What Causes Lumbar Spinal Stenosis (Especially at L4-L5)
Lumbar spinal stenosis most often develops gradually from age-related degenerative spinal changes, like disc degeneration, facet hypertrophy, osteoarthritis, thickened spinal ligaments, and spondylolisthesis. Though less common, other possible causes include spinal deformities (like scoliosis), congenital factors, and spinal trauma.
Disc and Facet Joint Degeneration
Intervertebral discs are cushion-like discs located between the vertebrae that act as shock absorbers. Facet joints are connection points between spinal bones that nerve roots pass through; they stabilize the spine while allowing it to bend, twist, and lean. Both spinal structures undergo significant wear and tear over time.
- Disc degeneration: Discs become thinner and drier over time, contributing to conditions like herniated disc and degenerative disc disease. Damaged discs can protrude into the spinal canal and may impinge on nearby nerves.
- Facet joint degeneration: Facet arthropathy, a type of spinal arthritis impacting the facet joints of the spine, can cause bone spurs, reducing the open space available for nerve roots to exit the spine.
Age-Related Canal Narrowing: Thickened Ligaments, Bone Spurs, and Synovial Cysts
Age-related spinal changes often contribute to the gradual development of spinal stenosis over time.
- Spinal ligaments tend to thicken and lose flexibility gradually over time, naturally reducing space in the spinal canal.
- Bone spurs, a common side effect of osteoarthritis, develop in response to joint damage. When they form in the spinal canal, they may cause stenosis.
- Synovial cysts are fluid-filled sacs that develop in the spine from age-related degeneration. Most synovial cysts occur at the L4-L5 level.
Other Causes: Spondylolisthesis, Spinal Deformities, Congenital Factors, and Trauma
Spondylolisthesis, a spinal condition resulting from a vertebra that slips down onto the vertebra below, can also cause L4-L5 stenosis. Spondylolisthesis is usually degenerative.
But while L4-L5 stenosis is usually caused by age-related wear and tear, it can also result from:
- Spinal deformities, like scoliosis
- Congenital factors, like being born with a narrow spinal canal (congenital spinal stenosis) and certain gene mutations
- Trauma to the spine, like vertebral fractures and dislocations
Who’s at Risk: Typical Demographics and Onset
People over age 50 are the most likely to experience stenosis from degenerative spinal changes. Its prevalence and severity rise with age, with lumbar spinal stenosis being one of the most common reasons for spinal surgery in older age.
Age 50 is often viewed as the age of onset, when stenosis starts to develop from age-related wear and tear, and the condition gradually progresses in the coming years and decades. According to a European Spine Journal study, as many as 80% of people show spinal narrowing on imaging tests (known as radiographic stenosis) by age 70, although not all are symptomatic.
Natural History: How L4-L5 Stenosis Usually Progresses
L4-L5 stenosis usually progresses slowly as the spine degenerates over time, often through these stages:
- Slow onset: The spinal canal gradually narrows as the spine slowly degenerates, often with no noticeable symptoms.
- Symptom development: The narrowing progressively impinges on nearby spinal nerves and nerve roots, triggering symptoms like neurogenic claudication.
- Mobility changes: As the stenosis worsens, standing, walking, and balancing may become a challenge.
- Severe L4-L5 stenosis: If the condition progresses to a severe stage, the patient may experience more intense neurogenic claudication and concerning symptoms, like leg weakness, foot drop, sexual dysfunction, and bladder and bowel changes.
Note that L4-L5 stenosis can progress to the point of appearing on imaging tests (radiographic stenosis), but remain asymptomatic, never advancing beyond the first stage. This is because symptoms may only develop if the stenosis causes nerve compression.
Classic Symptoms: Neurogenic Claudication and Positional Relief
Classic L4-L5 spinal stenosis symptoms fall under the umbrella of neurogenic claudication, a collection of symptoms associated with spinal nerve compression in the lumbar spine. Symptoms include:
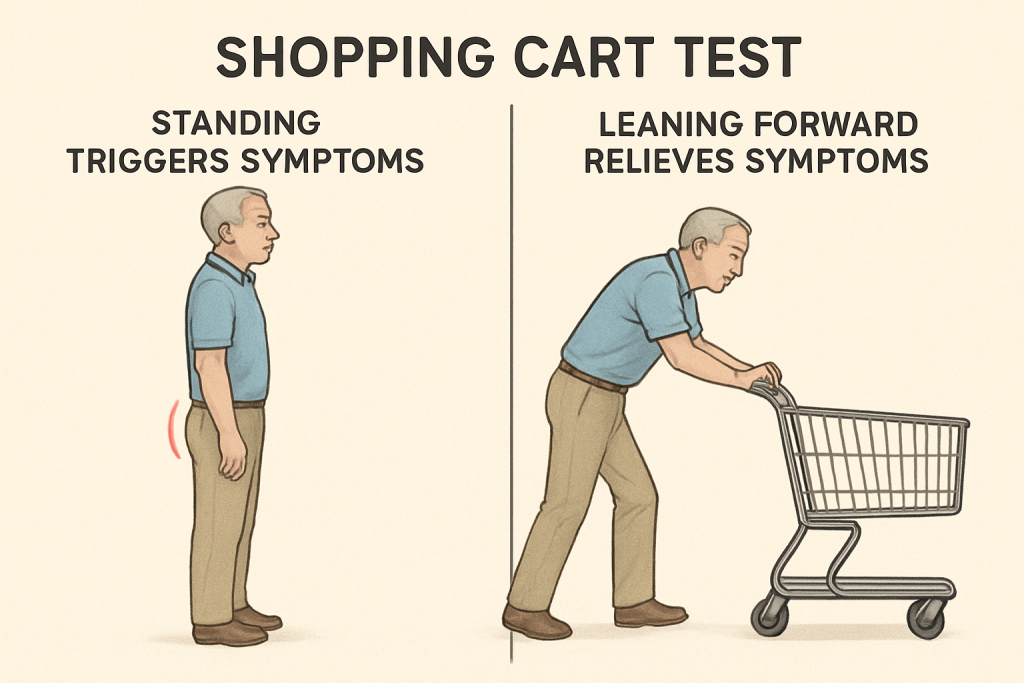
- Pain, numbness, tingling, and weakness in the lower back, leg(s), hip(s), or buttock(s) with standing, walking, and spinal extension (arching backward)
- Pain relief when sitting and leaning forward
- Inability to walk for extended periods
- Leg heaviness or cramping
L4-L5 stenosis is typically bilateral, meaning it affects both sides of the body, but asymmetrical, meaning your symptoms may differ in severity between sides of the body. Though less common, if the canal narrowing only occurs on one side, symptoms can present as unilateral.
The “shopping-cart sign” is a simple, informal test you can perform to see if your pain aligns with typical L4-L5 spinal stenosis symptoms. If your pain improves when you lean forward, as you would when pushing a shopping cart, but worsens when you stand upright, it might be neurogenic claudication. While this can help you better understand your symptoms, it’s not a replacement for medical care—make sure to schedule an appointment with your doctor if your symptoms persist for longer than a few weeks.
Severe Symptoms and Red Flags: When to Seek Urgent Care
If L4-L5 spinal stenosis becomes severe, it can cause radiculopathy and various “red flag” symptoms that require urgent care. Many of these symptoms point to cauda equina syndrome, which may cause permanent nerve damage if left untreated.
Radiculopathy refers to numbness, tingling, pain, or weakness that radiates from the spine into the extremities that the compressed nerve supplies (for L4-L5, this includes the knee, thigh, shin, and top of the foot). It’s typically manageable with conservative treatments and isn’t always considered a red flag symptom. But if you experience it, contact your doctor to schedule an appointment to prevent further nerve damage.
Red flag lumbar stenosis symptoms:
- “Foot drop” is a symptom resulting from weakness in the anterior tibialis muscle, most often caused by L4-L5 radiculopathy. It makes it difficult or impossible to point the ankle and toes upward, causing the foot to slap onto the ground while walking, with the leg dragging in front of the foot.
- What to do: Call your doctor to schedule an appointment.
- Sexual dysfunction or pain during intercourse
- What to do: Call your doctor to schedule an appointment.
- Bladder or bowel incontinence
- What to do: Go to the emergency room, as this is a possible cauda equina syndrome symptom.
- Severe weakness in both legs
- What to do: Go to the emergency room, as this is a possible cauda equina syndrome symptom.
- Saddle anesthesia: numbness in the genital and inner thigh area
- What to do: Go to the emergency room, as this is a possible cauda equina syndrome symptom.
When It’s Not Just L4-L5: Differential Diagnoses to Consider
Not all cases of lower back, leg, and buttock pain are lumbar stenosis. These symptoms can occur with other conditions, like vascular claudication, hip arthritis, and peripheral neuropathy.
- Vascular claudication stems from blood flow issues, causing pain or cramping in the legs during exercise. Here’s how it’s different:
- Relief: Vascular claudication pain improves with rest—stenosis improves with spinal flexion.
- Diagnosis: Vascular claudication presents with abnormal or absent peripheral pulses, with imaging showing narrowing of the leg arteries, often from plaque.
- Hip arthritis is characterized by hip joint inflammation, often from osteoarthritis. Here’s how it’s different:
- Symptoms: Hallmark hip arthritis symptoms include thigh or groin pain, hip stiffness, reduced hip mobility, and limping.
- Pain onset: Hip arthritis is often worse in the morning and with movement—stenosis pain worsens with standing, walking, and extension.
- Peripheral neuropathy is an umbrella term for conditions that damage the peripheral nervous system. Here’s how it’s different:
- Pain onset: Peripheral neuropathy pain tends to be constant, while stenosis pain worsens with walking.
- Pain location: Peripheral neuropathy pain doesn’t typically follow a nerve root pattern, while stenosis pain does.
- Imaging features: Peripheral neuropathy requires nerve conduction studies (NCS) to reveal abnormalities—stenosis patients often have near-normal NCS results.
Diagnosing L4-L5 Spinal Stenosis
L4-L5 spinal stenosis is typically diagnosed with a complete medical history, physical exam, functional tests (such as gait and reflex assessments and the “stoop test”), and imaging. EMG (electromyography) might also be used to identify nerve damage, although it’s not a routine diagnostic test for stenosis.
Patient History and Symptom Patterns
Your doctor will begin by gathering a complete medical history. This can help identify factors that may be contributing to your symptoms, like underlying medical conditions, past surgeries, and lifestyle factors. They’ll also ask questions about your symptoms, such as:
- How severe are your symptoms?
- How often do you experience symptoms?
- Do your symptoms occur with specific movements or postures?
- Is your pain worse at certain times of the day or night?
Your doctor will consider whether your symptoms follow the typical L4-L5 spinal stenosis patterns, meaning they worsen when you stand or walk and improve when you lean forward or sit (neurogenic claudication).
Physical Exam and Functional Tests: Stoop Test, Gait Load Test, Reflex/Sensation Tests
Your doctor will complete a comprehensive physical exam, during which they’ll check for signs of spinal stenosis using various functional tests, including:
- The stoop test evaluates if your symptoms improve when you bend forward, which points to stenosis.
- Gait assessments, like the Gait load test, evaluate if neurological symptoms impact your walking speed, stride, and stamina.
- Reflex/sensation assessments check for signs of nerve compression by prompting normal nerve responses and recording abnormalities.
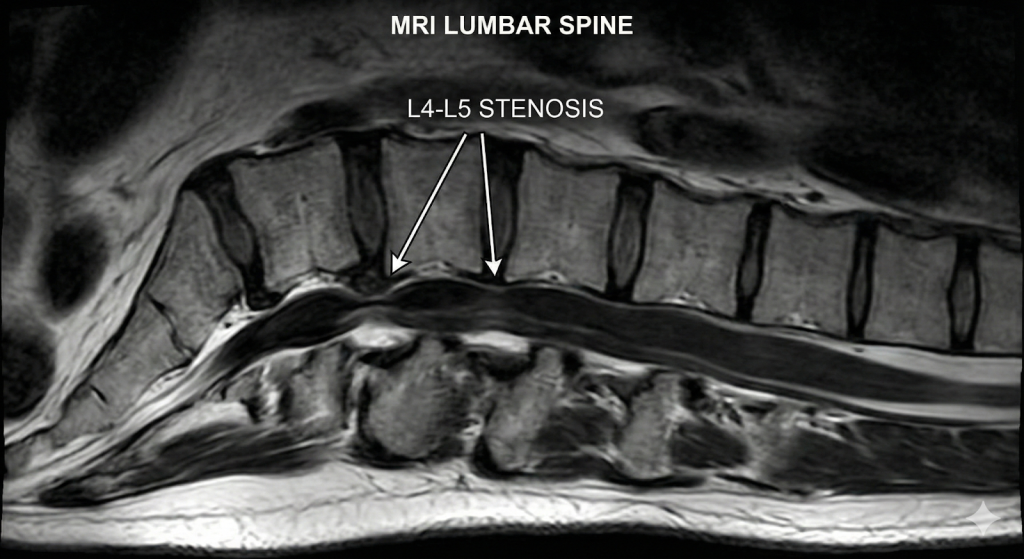
Imaging (X-Ray, MRI, CT/Myelogram) and EMG
If your exam indicates possible lumbar spinal stenosis, your physician may order imaging tests to view the spinal canal. Imaging tests that may be used to diagnose L4-L5 stenosis include:
- X-rays use electromagnetic radiation to create images of the inside of the body. They’re particularly helpful for visualizing bone tissue, so your doctor may use an X-ray to identify bone spurs, vertebral fractures, and other bone changes that can narrow the spinal canal.
- CT scans use a combination of X-rays and computer technology to create cross-sectional images of the body, allowing your doctor to view the spine in 3D. This can help pinpoint areas where the spinal canal has narrowed.
- MRIs (magnetic resonance imaging) use radio waves and magnetic fields to develop more detailed images of the body’s interior, including soft tissue. Unlike an X-ray, an MRI can reveal changes to the spinal nerves, discs, and other soft tissues, providing a more complete picture of the spinal stenosis.
Additionally, an electromyography (EMG) test can help paint a complete picture of spinal nerve damage. It records muscles’ electrical activity in response to nerve stimulation, which can help identify nerve damage or dysfunction, although it’s not as widely used to diagnose stenosis as the tests listed above.
It’s crucial to note that in some cases, spinal stenosis appears in imaging tests (radiographic stenosis), but the patient is asymptomatic or only mildly symptomatic.
Conservative and Non-Surgical Management
Conservative treatments for L4-L5 stenosis include posture management, activity adjustments, physical therapy, low-impact exercise, pain medications, steroid injections, walking aids, and weight management.
Posture and Activity Modification
Posture management for spinal stenosis involves keeping the spine in its natural alignment, often with a slight lean forward (flexion), which naturally opens up the spinal canal to alleviate nerve compression.
Activity modification involves avoiding movements, postures, and activities that flare up spinal stenosis symptoms, like spinal extensions, extended periods of walking or standing, and high-impact exercise.
Physical Therapy, Stretching, Strengthening Exercises
Physical therapy and exercises are effective non-invasive treatment options for L4-L5 stenosis, helping to improve both pain and physical function. An Annals of Internal Medicine study found that physical therapy is as effective as surgery for spinal stenosis, with fewer risks and complications.
Commonly recommended PT exercises for L4-L5 stenosis include:
- Pelvic tilts gently strengthen the core muscles without straining the spine.
- Bridges strengthen the core and glutes for overall stability.
- Planks are a full-body exercise that target the core and back muscles, which may help improve your posture.
- Knee-to-chest stretch can help you achieve spinal flexion, gently creating more space in the spinal canal to make you feel more comfortable.
- Seated lumbar stretch is a gentle way to gain more lumbar mobility while recovering from spinal stenosis.
Pain Management: Medications, Injections, Walking Aids
Pain management for L4-L5 stenosis often involves prescription medications to alleviate symptoms. According to Weill Cornell Medicine, options include:
- NSAIDs to reduce pain and inflammation
- Anti-seizure drugs (anticonvulsants) to alleviate nerve pain by regulating nerve signals
- Muscle relaxants to help with muscle spasms and pain
- Epidural steroid injections to reduce inflammation and calm pain
- Antidepressants to help with neuropathic pain in some patients
Alongside painkillers for stenosis, walking aids like wheeled walkers, canes, and even trekking poles can reduce impact on the lumbar spine and support balance, helping you move around safely.
Lifestyle Factors: Weight, Ergonomics, Exercise, Bone Health
- Reaching a healthy weight reduces impact on the spine during day-to-day activities.
- Improving ergonomics by adding lumbar support to chairs and raising computer screen heights to prevent slouching can help calm pain, especially for office workers.
- Low-impact exercises like swimming, walking, and aerobics can help you stay mobile without placing excessive stress on the lumbar spine.
- Supporting bone health can help when conditions like osteoporosis contribute to stenosis. Your doctor may suggest certain supplements, like calcium and vitamin D, as well as regular exercise.
Surgical and Interventional Options
Surgical treatment options for L4-L5 stenosis include spinal decompression procedures (laminectomy or microdiscectomy) with or without fusion, as well as spinal cord stimulation.
Conventional treatment options can’t reverse the narrowing of the spinal canal. Only surgery can provide the structural changes required to create more space in the canal and may be required if:
- Conventional treatment options fail to provide relief after six to 12 months
- You’re at risk of permanent neurological damage
- Your symptoms are severely disabling
Spinal Decompression Surgery: Laminectomy and Microdiscectomy
Surgery for spinal stenosis at the L4-L5 segment involves decompression techniques to relieve nerve compression. The most commonly used procedures are laminectomy and microdiscectomy.
- Laminectomy involves removing some or all of the lamina to create more open space in the spinal canal and alleviate nerve compression. The lamina is a small piece of bone that forms part of the vertebral arch, covering the back of the spinal canal.
- Microdiscectomy is a minimally invasive procedure to remove a portion of a slipped disc. It’s typically implemented if a damaged disc is causing the stenosis.
Spinal decompression can pose the risk of spinal instability. To negate this risk, these procedures are conventionally performed with spinal fusion.
- L4-L5 spinal fusion involves positioning bone graft material in between the L4 and L5 vertebrae, causing the vertebrae to permanently fuse over several months and eliminating motion at the fused segment.
David danced at his son’s wedding Bonnie explains why TOPS surgery was the right decision for her Wade is back to hiking Scott speaks about going to surgeryInspired by motion, driven by innovation




Regain your mobility with Premia Spine! Contact us now
Decompression with Fusion: Considerations
Refer to this table to consider the risks and outcomes of decompression with fusion vs. decompression alone for L4-L5 spinal stenosis:
| Decompression with Fusion | Non-Fusion Decompression | |
| Hospital Stay | ~4 days | Shorter, often 1 to 3 days |
| Recovery Time | 4 to 6 weeks to return to light activity; up to a year for a full recovery | 2 to 4 weeks to return to light activity |
| Spinal Motion | Eliminates motion at the fused segment | Preserves the spine’s natural motion at the operated level |
| Risk of Recurrent Symptoms | Risk of adjacent segment disease (ASD) and failed fusion (pseudoarthrosis) | Risk of spinal instability |
| Success Rate* | 24% | 77% |
*according to the TOPS System clinical study
Spinal Cord Stimulation and Other Alternatives
Non-fusion spinal implants like the TOPS System and spinal cord stimulation are alternatives to conventional surgery for severe L4-L5 stenosis.
The TOPS System from Premia Spine is an advanced, FDA-approved, non-fusion implant that replaces the tissues removed during lumbar decompression. It stabilizes the spine without compromising its natural motion in all directions, allowing patients to return to all of their usual activities within a faster recovery period, without the risk of adjacent segment degeneration.
Spinal cord stimulation (SCS) involves implanting a device that sends low-grade electrical currents to the spinal cord, helping to block pain signals to the brain. A Neuromodulation study found SCS to be effective at treating chronic pain from lumbar spinal stenosis.
What to Expect: Recovery and Risks
Recovery after L4-L5 lumbar stenosis surgery involves activity modification, physical therapy, and low-impact exercise. Lifestyle adjustments, like eating a nutritious diet and limiting alcohol consumption, can further support recovery.
- Activity modifications will fluctuate as you recover. In the earliest healing stages, your movements will be relatively limited, and you’ll be advised to avoid stretching, twisting, or bending the spine. But it’s also important to avoid prolonged bed rest, as it can strain the spine and contribute to weakened muscles.
- Physical therapy helps you regain strength and mobility through targeted exercise, stretches, and complementary treatments. Your PT can also correct imbalanced movement patterns that could slow your recovery.
- Low-impact exercise promotes circulation, muscle strength, and flexibility during stenosis surgery rehabilitation. Options include walking, swimming, and water aerobics, although your PT can provide personalized recommendations.
Though rare, risks to consider after surgery for L4-L5 spinal stenosis surgery include:
- Infection
- Warning signs: Fever, redness and warmth around the incision
- Deep vein thrombosis
- Swelling, pain, or tenderness in one calf
- Neurological injury
- Warning signs: New or worsening weakness, numbness, or tingling; bladder or bowel function changes
- Spinal fluid leak
- Severe headaches, nausea, or dizziness
Long-term risks associated with spinal fusion include failed fusion and adjacent segment disease. If your symptoms return or persist beyond the typical healing period, schedule an appointment with your spine specialist.
Prognosis & Long-Term Outlook: What Patients Need to Know
The prognosis and long-term outlook for patients with severe spinal stenosis are generally positive, especially when they receive prompt care and adhere to the prescribed treatment plan. It’s possible to live a normal or near-normal life with lumbar spinal stenosis, although outcomes vary between conservative and surgical treatment plans.
| Conservative Treatment (physical therapy, medications, steroid injections) | Surgical Treatment(surgical decompression with laminectomy or discectomy) | |
| Pain Relief | ModestIdeal for mild-to-moderate pain | RobustUsually effective, even for severe symptoms |
| Mobility | Gradual improvement, often with long-term restrictions | Faster improvement, sometimes with long-term restrictions |
| Long-Term Risks | Risk of progressive (potentially permanent) nerve damage | Risks associated with surgery and anesthesia, including infection, blood clots, and dural tearRisk of reoperation (rates range from 11% to 18%) |
Here are other factors to consider:
- Exercise: Most people can return to most forms of exercise after spinal stenosis surgery, especially those who stick to minimally invasive procedures. Research shows that patients who exercise before and after spine surgery recover more effectively and are mentally healthier than those who don’t.
- Healthy habits: It’s possible to improve the long-term outlook on severe spinal stenosis by adopting healthier habits. An anti-inflammatory diet, low-impact exercise, social connections, and stress management can all support your body’s ability to heal.
Prevention and Spine Health: How to Reduce Risk or Slow Progression
Protecting your spinal health with these adjustments can help slow the progression of L4-L5 spinal stenosis before it becomes severe:
- Lifestyle changes like eating a nutritious diet, drinking less alcohol, and quitting smoking
- Posture improvements while sitting, standing, and exercising
- Ergonomic workplace adjustments, like purchasing a chair with robust lumbar support
- Weight management
- Low-impact exercise, including stretching and strengthening exercises
- Bone and joint health preservation with strength training and potentially calcium and vitamin D supplementation (if advised by your doctor)
- Periodic monitoring to catch symptoms in their early stages, before they become severe
FAQ: Common Questions About L4-L5 Spinal Stenosis
- Can I have L4-L5 stenosis without back pain?
- Yes, this is known as asymptomatic stenosis.
- Is foot drop permanent?
- Not always—many cases are reversible with treatment.
- Is imaging enough to diagnose L4-L5 spinal stenosis?
- No, your doctor will need to evaluate your symptoms and perform a physical exam to diagnose symptomatic stenosis.
- Can I exercise with stenosis?
- Yes, low-impact exercise is recommended for stenosis to preserve mobility.
- What are the final stages of spinal stenosis?
- Severe, debilitating back and leg pain, severely restricted mobility, and severe neurological symptoms.