



L4-L5 Fusion Success Rate: Clinical Data & Recovery Guide
L4-L5 spinal fusion success rates typically range from 65% to over 90%, depending on the patient’s age, underlying medical conditions, and overall health, as well as the applied surgical approach. While fusion effectively stabilizes the spine after decompression for spinal stenosis, spondylolisthesis, degenerative disc disease, and other spinal conditions, it’s crucial to evaluate the risk of fusion failure, adjacent segment disease, hardware failure, and recurring pain.
In this comprehensive guide, we’ll review the clinical success rates for L4-L5 fusion, typical recovery timelines, potential risks, and modern alternatives to achieve stability without compromising mobility.

What’s the Real Success Rate of L4-L5 Fusion?
The real success rate of L4-L5 fusion is 65% to over 90%, according to a Seminars in Plastic Surgery study. This percentage varies based on patient age, underlying medical conditions, bone graft material, number of fused levels, and surgical approach.
| Quick Stats: L4-L5 Fusion Success Rate | ||
| Condition | Success Rate | Source |
| Degenerative spondylolisthesis | 92% improved after surgery, 90% were very satisfied with their results | Indian Journal of Orthopaedics |
| Lumbar spinal stenosis | 78% (22% reoperation rate) | The New England Journal of Medicine |
| Recurrent disc herniations | 92% improved after surgery 90% were very satisfied with their results | Journal of Neurosurgery |
Factors That Determine Your Personal Success Rate
These factors can reduce the chance of success in L4-L5 lumbar fusions:
- Smoking or using other nicotine products
- BMI and obesity
- Low bone density, possibly due to osteoporosis
- Certain chronic conditions, like diabetes and rheumatoid arthritis
- Poor nutrition, particularly not consuming enough protein
- Engaging in strenuous activities during the recovery process
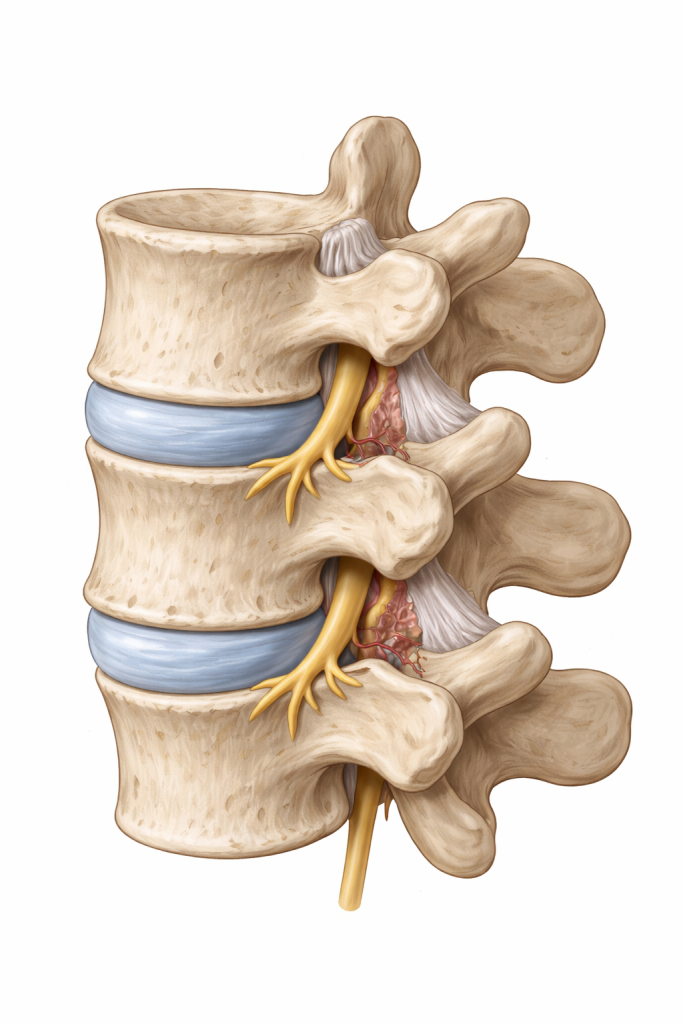
L4-L5 Fusion: Surgical Overview
L4-L5 fusion involves fusing the L4 and L5 vertebrae in the lumbar spine. It’s commonly performed to treat lumbar spine conditions, including spinal stenosis, spondylolisthesis, disc degeneration, vertebral fractures, and herniated discs.
The spine consists of four sections: the cervical spine (the neck), the thoracic spine (the mid-back), the lumbar spine (the lower back), and the sacral spine (directly above the tailbone). Each of the vertebrae of the spine has been assigned a letter and a number according to these sections. The lumbar spine includes the L1 through the L5 vertebrae.
Spinal fusions are most commonly performed on the lumbar spine. Over 300,000 lumbar spine procedures are estimated to be performed in the United States each year, according to an American Journal of Neuroradiology study.
The Steps of L4-L5 Fusion
An L4-L5 fusion surgery overview involves the following steps:
- Make the incision.
- Access the L4-L5 spinal level.
- Remove the damaged disc material.
- Prep the disc space.
- Position the bone graft.
- Insert hardware, if required.
- Close the incision.
The surgeon must make an incision to access the L4-L5 segment. The incision is made in the back, front, or side of the body, depending on the surgical approach.
- Transforaminal lumbar interbody fusion requires an incision in the back.
- Anterior lumbar interbody fusion requires an incision in the abdomen.
- Extreme lateral interbody fusion requires an incision in the side of the body.
Preoperative Prep for L4-L5 Fusion
Before arriving at the hospital on surgery day, you’ll need to take several steps to ensure a safe, successful L4-L5 fusion, including medical tests, medication adjustments, and lifestyle habit shifts. While your surgical team will provide detailed pre-op instructions for your particular situation, you can consider these general guidelines:
- Tests: You’ll likely be required to complete various medical tests to ensure you’re in good enough physical health for surgery. Examples include blood testing, an electrocardiogram (EKG), and a chest X-ray.
- Medications: You’ll need to stop taking any medications that can thin your blood seven to 10 days before surgery. Common examples include aspirin, NSAIDs, blood thinners, antiplatelets, and certain herbs and supplements, including fish oil and vitamin E.
- Smoking: It’s crucial to quit smoking as soon as possible before spinal fusion, as smoking contributes to reduced fusion success rates and a higher risk of complications.
- Lifestyle adjustments: Along with quitting smoking, adjusting your lifestyle to include a nutritious diet, little to no alcohol, and low-impact exercise will set your body up for success before fusion. Your surgeon may advise you to work toward specific goals, like reaching a healthy weight, before undergoing the procedure.
What Happens During L4-L5 Fusion Surgery?
Understanding what happens during L4-L5 fusion surgery can help you feel confident and informed leading up to the procedure. While the exact details of the surgery will vary depending on the surgical approach, fusion typically involves these steps:
Pre-Op Prep
First, you’ll arrive at the hospital on the day of your procedure and begin the pre-op process. This involves completing any required paperwork, changing into a hospital gown, and getting situated in an exam room. A hospital nurse will check your vitals before your surgeon and anesthesiologist will meet with you to provide a surgery overview and answer any lingering questions.
Anesthesia
Spinal fusion is typically performed under general anesthesia, meaning you’ll be asleep for the procedure. First, you’ll be given anti-anxiety medications to help calm you down. Then, you’ll be taken to the operating room, and the anesthesiologist will place an IV line to administer the anesthesia. Patients usually fall asleep within two minutes.
Incision
After the anesthesia has kicked in, the surgery can begin. Your surgeon will make an incision in the back, side, or front of the body, depending on the type of fusion being performed.
Gaining Access to the Spine
After making the incision, the surgeon may need to separate the back muscles (in transforaminal lumbar fusion) or move the peritoneum aside (in anterior lumbar and extreme lateral interbody fusion). The peritoneum is the sac that surrounds the organs in the abdomen.
Removing Disc Material
With access to the L4-L5 level, the surgeon removes the damaged intervertebral disc. The empty disc space is then prepped and measured for the spacer, which contains bone graft material.
Placing the Graft Material
Once ready, the spacer is inserted into the disc space. If necessary, it may be secured into place with hardware, like plates, rods, and screws. This hardware offers additional stability as the bone graft heals.
Closing the Incision
With the bone graft anchored in place, it’s time to close the incision. The surgeon removes their instruments, returns the back muscles or peritoneum to their normal position, and uses sutures to close the incision.
Waking Up
After L4-L5 fusion, you’ll wake up in the hospital’s recovery area. Most patients remain in the hospital for at least 24 hours after the procedure before returning home. In the hospital, a physical or occupational therapist will help you complete basic movements and advise you on activities to avoid during the recovery process.
Types of L4-L5 Fusion Surgery
The primary types of fusion surgery are PLIF, TLIF, ALIF, and XLIF, all of which involve different surgical approaches. Your surgeon will determine the best approach for your needs based on your body, medical condition, and goals for the procedure.
- PLIF (posterior lumbar interbody fusion)
- Performed through an incision in the center of the back
- Considered the traditional approach to lumbar fusion
- Requires the surgeon to cut through the large back muscles and retract nerve roots to reach the spine
- Causes more tissue disturbance and post-op pain
- TLIF (transforaminal lumbar interbody fusion)
- Performed through an incision in the lower back
- Accesses the vertebra from the side
- Surgeon removes the facet joints from the vertebra to access the spine through the intervertebral foramen (a bony opening situated on either side of the spinal column at every spinal level)
- ALIF (anterior lumbar interbody fusion)
- Performed through an incision in the front of the body
- Surgeon makes an incision in the belly, spreads the abdominal muscles, and moves the peritoneal sac (which holds the intestines) to one side
- Avoids back muscle and nerve disturbance
- XLIF (extreme lateral interbody fusion)
- Minimally invasive form of spinal fusion
- Surgeon reaches the spine through the side of the body
- Eliminates the need to cut through the back muscles or move the abdominal organs
The L4-L5 Fusion Recovery Timeline (Milestones)
Spinal fusion recovery occurs in stages, from the early postoperative period to the final phases of healing, typically taking six to 12 months for a full recovery.
Recovering in the Hospital
You may need to remain in the hospital for up to four days after spinal fusion surgery (or longer for people with a higher risk of serious complications, like infections). While there, your healthcare providers will continually check your pain levels, making sure the procedure was successful. You may also consult with a physical therapist to learn how to safely complete basic tasks, like standing, walking, and getting dressed.
Week 1 and 2
During this early period, it’s crucial to follow all of your aftercare instructions, from caring for the wound to keeping your spine stable. You may also be prescribed medications for pain.
During this time, you’ll be advised to avoid spinal bending and twisting, lifting any objects heavier than around eight pounds, and strenuous physical activity. You’ll also need to remain home from work.
To gain mobility and avoid prolonged bed rest, your surgeon and PT will likely recommend walking in the first two weeks after fusion.
- During week one, aim to walk in short bursts of five to 10 minutes, multiple times each day.
- During week two, aim to increase the walk duration to 10 to 15 minutes, at least twice daily.
Walk on flat surfaces while wearing supportive shoes. Avoid bending or twisting, and stop if you experience pain beyond the typical post-op discomfort.
The log roll technique can help you get in and out of bed safely in this early recovery stage:
- Stand with the backs of your legs against the bed.
- Bend your knees while reaching your hands back toward the bed.
- Using your arms, lower yourself gently to sit on the side of the bed.
- Keeping your spine straight, without twisting or bending, lower your upper body to the bed while raising your legs, keeping them aligned with your torso.
- Once lying sideways on the bed, consider placing a pillow between your knees for extra support.

Weeks 3 to 12
Your vertebrae are actively fusing, and you’ll rely on physical therapy appointments to build muscle strength, regain flexibility, and support the recovery process. Post-fusion PT typically focuses heavily on core stabilization to alleviate impact on the spine. Your PT will also tell you which forms of exercise are safe, such as walking and water aerobics.
You’ll gradually return to day-to-day chores and activities, including driving. People with non-active jobs typically return to work during this period. However, you’ll need to keep steering clear of spinal bending, twisting, and heavy lifting.
6 Months and Beyond
After around six months, you’ll check in with your surgeon to ensure the vertebrae fused successfully. If everything looks good, you’ll be cleared to return to most of your normal activities, including non-extreme spinal twisting, bending, and lifting. Individuals with more active jobs can usually go back to work at this point.
About a year after spinal fusion, most patients feel fully recovered, with complete relief from their back pain. You may have some permanent mobility restrictions at the fused level.
How Long Does it Take to Recover from L4-L5 Fusion?
It takes between six months and one year to fully recover from L4-L5 fusion.
- Return to housework: You may need four to six weeks to return to basic activities around the house.
- Work:
- Sedentary: One to two months off
- Light physical activity: Three to six months off
- Hard physical labor: May require a career pivot
Fusion requires such a lengthy recovery process because it involves bone healing. Bone tissue takes longer to heal than soft tissue.
Dietary Needs for Bone Fusion: Calcium, Vitamin D, and Protein
Adjusting your diet to contain adequate amounts of calcium, vitamin D, and protein can support your body’s recovery after fusion.
- Calcium supports overall bone health and new bone formation. A Journal of Korean Neurosurgical Society study found that calcium intake increased fusion mass volume and mechanical strength.
- Vitamin D improves calcium absorption and prevents bone loss. A BMC Musculoskeletal Disorders study found that vitamin D supplementation resulted in shorter fusion times, better spine function, and less post-fusion pain.
- Protein preserves muscle mass and regeneration after spinal fusion, according to an International Spine Journal of Surgery study.
Sexual Activity and Social Life After Lumbar Fusion
Maintaining an active sexual and social life after lumbar fusion is essential to preserving your quality of life.
- Patients are typically advised to wait a few weeks after fusion before engaging in normal sexual activity. But make sure to:
- Stop if you experience pain.
- Avoid any twisting, bending, or lifting.
- Seek guidance if you experience problems.
Here’s the good news: Patients surgically treated for chronic back pain report having better sex lives than those non-surgically treated, according to a European Spine Journal study. Just be sure to be patient and focus on your recovery.
- Your social life will look a bit different in the first few months after spinal fusion. You may experience:
- Increased reliance on others for basic support
- Reduced ability to participate in active social activities, like sports
- Emotional ups and downs related to recovery
- Reduced alcohol intake as you prioritize post-op nutrition
Maintaining social connections can tremendously help your mental health and overall healing process. To avoid feelings of isolation, reach out to loved ones often. Adjust meet-ups to include activities you can participate in, like taking short walks or even serving as a scorekeeper until you recover.
Physical Therapy and Rehabilitation After Spinal Fusion
Physical therapy and rehabilitation are essential pieces of the recovery puzzle after L4-L5 fusion. PT will help you regain strength and mobility while your body recovers through targeted exercises, stretches, and complementary therapies.
Surgeons often advise starting physical therapy within one to three months of the surgery. A 2017 study found that starting PT 12 weeks post-op led to better outcomes and lower costs than starting PT after six weeks.
Common post-fusion PT exercises include:
- Pelvic tilts and bridges, which engage the deep core muscles to build stability
- Seated marching, another gentle core exercise that promotes overall function

- Leg slides and straight leg raises
- Hamstring stretches
- Short walks, gradually increasing the distance as you gain endurance
Long-term rehab for L4-L5 fusion patients often involves a self-managed activity program, including exercises and stretches from a PT. Your PT can transition you to this independent approach once you’ve effectively recovered from the procedure. If you experience any recurring pain or neurological symptoms, you may need to return to the PT for further support.
Common Challenges and How to Manage Them
Common challenges post-fusion include pain management, mobility, and constipation.
Managing Pain Medications
| Post-Fusion Pain Management | |||
| Acetaminophen | NSAIDs | Narcotics/Opioids | |
| Mechanism of Action | Altering the brain’s pain perception & temperature regulation | Block enzymes to prevent the production of chemicals that cause pain & inflammation (prostaglandins) | Activate opioid receptors in the brain to block brain signals between the brain & body |
| Examples | Acetaminophen/Tylenol | IbuprofenNaproxenKetorolacCelecoxib | MorphineOxycodoneHydrocodoneMethadone |
| Risks | Liver damage (if taken in excess) | Opioid dependence Slowed wound healing | Opioid dependenceSlowed wound healing |
Managing Constipation and Mobility
Anesthesia, pain medication, and being sedentary can lead to constipation after spinal fusion. To manage this, try to:
- Hydrate
- Up your fiber intake
- Lower your intake of processed foods and dairy
- Get up and walk around for a few minutes, several times per day
- Stick to a routine to keep your bowel movements regular
- Sip a cup of morning coffee to induce the urge to go
To manage reduced mobility after fusion:
- Adhere to your recommended physical therapy protocol
- Take short, frequent walks
- Practice core strengthening exercises
- Ease into a low-impact exercise regimen while avoiding twisting, bending, and lifting
Preparing Your Home for Post-Op Life
After L4-L5 spinal fusion, basic tasks around your house may be extremely difficult. To combat this, ask a loved one to stay with you for support during the first few weeks, and take the following steps to prepare your home:
- Move items in your kitchen and bathroom off the high shelves so that you won’t have to strain to reach them.
- Stock your kitchen with nutritious, ready-made meals so that you don’t have to worry about cooking while you recover.
- Do all of your laundry and set out comfortable clothes to wear during the early stages of your spinal fusion recovery.
- Consider purchasing assistive tools to simplify your routine, like:
- Walker or cane
- Grabber tool
- Bed rail
- Shower chair
- Toilet riser
- Handheld showerhead
Risks and Potential Complications: Beyond the Basics
Beyond the risks associated with all surgical procedures (infection at the surgical site, thrombosis, and complications from anesthesia), the risks of L4-L5 spinal fusion include:
- Fusion failure (pseudoarthrosis)
This occurs when the vertebrae fail to properly fuse. Many factors can contribute to pseudoarthrosis, including smoking, infection, insufficient blood flow, excessive movement at the fusion site, osteoporosis, and malnutrition.
One study reported that pseudoarthrosis occurs in at least 15% of primary lumbar fusions. Though this complication is typically associated with lower back pain or radicular pain, it can be asymptomatic.
- Adjacent segment disease (ASD)
This complication results from excessive wear and tear on the spinal levels above and below the fused segment. This occurs because the adjacent vertebrae must compensate for the lost mobility in the fused segment.
ASD occurs in up to 30% of lumbar spine surgery cases, according to a Surgical Neurology International study, and a Clinical Spine Surgery review found that between 2% to 4% of spinal fusion patients per year experience ASD.
ASD symptoms often include:
- Back pain
- Pain that radiates from the back into the legs and/or feet
- Numbness, tingling, and/or weakness in the legs and/or feet
- Trouble standing
- Pain while walking
Considering its prevalence, fusion patients may want to proactively avoid ASD as they recover from surgery. To do so, consider these ASD risk factors:
- Being over age 60
- BMI over 25kg/m2
- History of smoking
- Pre-existing spinal degeneration
- Underlying medical conditions, including osteoporosis and rheumatoid arthritis
- Post-menopause stage
- Hardware failure
Pedicle screws, rods, spacers, and cages are all types of hardware commonly used in spinal fusion. This hardware can degenerate or even break over time, especially if the spine is subject to significant stress and impact. Worn-out or broken hardware can lead to recurrent spinal pain, along with neurological symptoms.
A Journal of Neurosurgery study reported a symptomatic hardware failure rate of 20% after instrumented fusion for metastatic disease. Other studies have reported rates as low as 3%.
When to Call Your Surgeon: Post-Op Red Flags
If you experience any of these symptoms after spinal fusion, call your surgeon immediately:
- New numbness, weakness, or tingling
- Worsening pain
- Incision opening
- Fever
- Redness, swelling, warmth, or abnormal drainage from the incision
If you experience any of these red flag symptoms after fusion, seek emergency medical care:
- Loss of bowel or bladder control
- Saddle anesthesia (numbness in the inner thighs, buttocks, and perineum)
- Sudden, severe weakness or other neurological symptoms
- Chest pain
- Shortness of breath
Long-Term Outlook: Life 5 to 10 Years After Fusion
Five to 10 years after spinal fusion, the goal is to be pain-free and mobile with a high quality of life. While this is the reality for some, others experience new or recurrent pain due to adjacent segment disease or hardware failure. A Global Spine Journal study reported a 17.5% rate of revision surgery five years after spinal fusion for lumbar stenosis.
To improve the long-term outlook for your spinal fusion, you can:
- Follow all of your surgeon’s pre-and post-op guidance
- Quit smoking and limit alcohol intake
- Optimize your nutrition, focusing on essential nutrients (including calcium, vitamin D, and protein)
- Stay active with low-impact, gentle movement that omits all spinal twisting, bending, and heavy lifting
- Attend all recommended follow-up appointments and PT sessions
Modern Alternatives: When Fusion Isn’t the Only Answer

Fusion isn’t the only solution for L4-L5 spinal conditions. The TOPS™ System is a modern alternative: an FDA-approved mechanical device made to be implanted between the L2 and L5 segments for degenerative spondylolisthesis and lumbar spinal stenosis.
David danced at his son’s wedding Bonnie explains why TOPS surgery was the right decision for her Wade is back to hiking Scott speaks about going to surgeryLive an active lifestyle again starting Now!



Regain your mobility with Premia Spine! Contact us now
TOPS™ stabilizes the spine without eliminating the independent motion of the spinal segments by replacing the tissues removed during decompression surgery.
L4-L5 Fusion vs. TOPS™: A Comparative Success Analysis
The TOPS™ System has an overall clinical success rate of 77%, compared to a rate of 24% for spinal fusion, according to the TOPS™ U.S. clinical trial.
| Pros | Cons | |
| TOPS™ System | Longstanding procedure, Protection against instability & spinal deformities, Restored spinal alignment, Pain relief | Newer procedure |
| Spinal Fusion | Invasive, long recovery period & hospital stay. Risk of pseudoarthrosis, ASD, and permanently reduced spinal mobility | Invasive, long recovery period & hospital stay. Risk of pseudoarthrosis, ASDPermanently reduced spinal mobility |
FAQs
- How should I wash my hair after spinal fusion surgery on L4-L5?
- Use a hand-held shower head. If you don’t have one, bend at the knees and waist to fit your head under the shower head. Make sure not to arch your back to wash your hair after fusion.
- What percentage of back fusions fail?
- 10% to 46% of lumbar spine surgery fails, according to an Asian Spine Journal study.
- How risky is lumbar fusion surgery?
- Lumbar fusion comes with certain risks, including bleeding, reactions to anesthesia, infection, nerve damage, failed fusion, adjacent segment disease, and recurrent pain. The riskiness of the procedure is largely impacted by your age, medical condition, and the invasiveness of the fusion approach.
- What is the hardest part of lumbar fusion recovery?
- The hardest part of lumbar fusion recovery is often post-op pain, which can make it difficult to participate in daily activities.
- How many hours is lumbar fusion surgery?
- It typically takes between one and seven hours. Minimally invasive fusion is quicker, while open surgery takes longer.
- How many years does a lumbar fusion last?
- Lumbar fusion is intended to be permanent and last a lifetime, but it increases the impact on the surrounding spinal segments and can cause adjacent segment degeneration over time. It’s often not recommended in younger patients who have decades left in their lifespan and are more likely to experience adjacent segment degeneration.