



How to Sit and Sleep with Spondylolisthesis: Best Positions & Tips for Pain Relief
If you have symptomatic spondylolisthesis, you likely know that the condition can make it difficult to sit and sleep comfortably.

Below, you’ll find clear guidance you can use tonight and the “why” behind each tip so you can tailor it to your body.
What Is Spondylolisthesis?
Spondylolisthesis occurs when one vertebra slips forward over the one below it, most commonly at L4-L5 or L5-S1.

That slippage can narrow spaces where nerves travel, leading to lower back pain, stiffness, or sciatica-like leg symptoms. Many people live full, active lives with it – especially when they optimize posture, sleep, and strength. Spondylolistheis severity is graded I-V; treatment is tailored to symptoms, function, and imaging.
Symptoms and Causes: Why Your Back Acts the Way It Does
When a segment slips, your body often compensates by tightening hamstrings and back muscles to stabilize the area. That protective tension can create a “stiff, achy” loop – especially after long sitting or in the morning.
- Common symptoms: aching low back, pain with standing/extension, leg pain or numbness, tight hamstrings, relief when flexing forward (e.g., leaning on a cart).
- Typical causes: age-related changes (degenerative), stress fracture (isthmic), congenital alignment differences, trauma, or repetitive hyperextension from sports.
Summary
Spondylolisthesis is a condition where one of the vertebrae in the spine becomes displaced due to instability, moving downward from its proper position and settling on the vertebra beneath it. This malpositioning can put pressure on the spinal cord and the nerves that emanate from the spinal column.
Spondylolisthesis causes pain and discomfort when one of the vertebrae (bones in the spine) moves out of its natural position. It most commonly occurs in the lumbar region (lower back), specifically at the L5-S1 level of the spine, followed by the L4-5 level.
Read more:
What is Spondylolisthesis?
Grade 1 Spondylolisthesis: Causes, Treatments, Recovery Forecasts
Grade 2 Spondylolisthesis
How I Cured My Spondylolisthesis Naturally?
Spondylosis vs. Spondylolysis vs. Spondylolisthesis: Key Differences and Treatment Options
Spondylolisthesis in Athletes: Treatment and Return to Sports
L4-L5 Spondylolisthesis
Best Sleeping Positions for Spondylolisthesis
Sleep is your daily reset. The goal is a neutral spine that unloads the slipped level and calms irritated nerves. Small setup tweaks often flip the switch from restless to restorative sleep.
Back sleeping with knee support

- Place a pillow beneath your knees to gently reduce lumbar extension.
- Keep your pelvis neutral – if your low back arches, add height to the pillow.
- Use a head pillow that keeps your neck aligned, not propped forward.
Why it works: Elevating the knees reduces shear forces and facet joint compression, which can ease radicular symptoms.
Reclined sleep (adjustable bed or wedge)

- Slightly elevate your torso and knees; aim for a “zero-gravity” feel.
- A wedge under the torso plus a second under the knees can mimic an adjustable base.
Why it works: Mild hip and knee flexion opens the neuroforamina and reduces load on the posterior elements – often relieving leg pain.
Side sleeping with a knee pillow

- Keep hips stacked; place a pillow between knees and ankles to prevent pelvic rotation.
- If your waist “drops” into the mattress, use a small waist support.
Why it works: The pillow keeps your pelvis from twisting, protecting the segment from rotational stress overnight.
Positions to limit
- Stomach sleeping increases lumbar extension; if unavoidable, place a thin pillow under the hips to blunt the arch.

Sleep-Friendly Add-ons:
- Try a breathable knee pillow to reduce tossing and turning.
- Test mattress firmness: medium to medium-firm often supports neutral alignment better than very soft beds.
Summary
Below is the structured table categorizing sleeping positions, their setup/technique, associated benefits, and relevant notes.
| Sleeping Position | Setup/Technique | Benefits | Notes |
|---|---|---|---|
| Back Sleeping | Use a pillow under the knees | Reduces lumbar extension, maintains neutral pelvis | Helps maintain neutral spine and reduces shear forces; ideal for minimizing spinal strain |
| Reclined / Zero-Gravity | Use an adjustable bed or wedges to recline | Opens neuroforamina, reduces nerve compression | Alleviates nerve pressure and improves sleep quality; highly effective for spinal decompression |
| Side Sleeping | Place a pillow between the knees, keep hips stacked | Prevents pelvic rotation | Ensures proper alignment; use a breathable knee or body pillow to reduce nighttime movement |
| Stomach Sleeping | Avoid if possible; if unavoidable, place a thin pillow under the hips | Minimizes increased lumbar extension | Increases lumbar extension and neck strain; can exacerbate slippage; modification reduces risk |
| General Tips | Use a medium to medium-firm mattress and supportive pillows | Supports spinal alignment | Enhances comfort, reduces pain, and promotes consistent posture throughout the night |
| General Benefits (across positions) | Proper positioning during sleep | Maintains neutral spine, reduces shear forces, alleviates nerve pressure, improves sleep quality, decreases pain | Apply to all recommended positions; consistent practice yields best long-term outcomes |
Read More:
Spondylolisthesis Self-Care: Effective Pain Management Techniques for Daily Relief
Spondylolisthesis Exercises Guide
How to Adjust Your Lifestyle for Faster Recovery from Spondylolisthesis Treatment Surgery
Best Sitting Postures for Spondylolisthesis
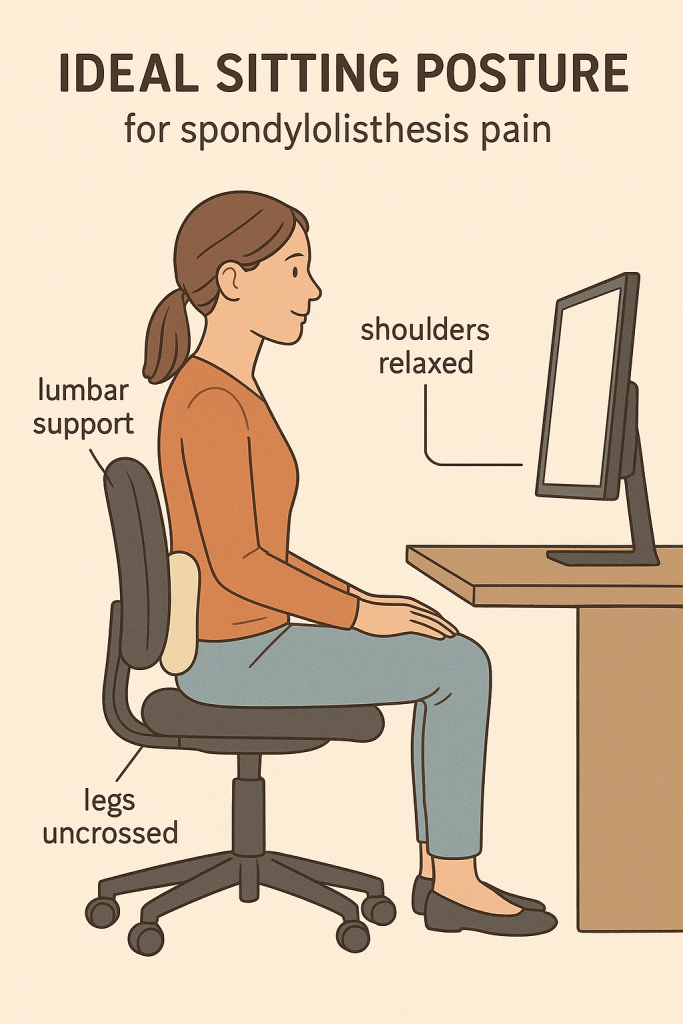
If you have spondylolisthesis, sitting with good posture in a chair with adequate lower back support is ideal for pain prevention. Good posture while sitting involves keeping your back straight, with your shoulders back and relaxed. If you’re working on a computer, the screen should be positioned at eye level so that you don’t have to tilt your head up or down.
Placing a rolled-up towel or a lumbar roll pillow behind your lower back can help you sit comfortably in chairs without enough support. Additionally, make sure to keep your hips level and your legs uncrossed while you sit to keep your lumbar spine aligned.
Sitting isn’t “bad,” but static, slouched sitting often is. Think alignment plus movement.
Your quick setup checklist
- Feet supported: flat on floor or on a footrest; knees level with or slightly below hips.

- Hips back in the chair with lumbar support (built-in or a small cushion).

- Slight recline (about 105-110°) reduces disc and facet loading compared to upright 90° sitting.

- Screen near eye level; elbows ~90°, shoulders relaxed to prevent creeping forward.
Make it dynamic
- Change positions every 20-30 minutes. Micro-breaks as little as 30-60 seconds help.
- Alternate sit/stand if available; even two 5-minute standing breaks per hour can reduce discomfort.
- Gentle micro-movements – pelvic tilts, shoulder rolls, ankle pumps – keep tissues perfused.
Sitting in a Car

- Use a small lumbar roll and a slight backrest recline.
- Slide the seat forward to avoid reaching and over-arching.
- On long trips, break every 45-60 minutes for a brief walk and hip flexor stretch.
Summary:
The following are the core practical guidelines for sitting with spondylolisthesis to help reduce pain and spinal stress:
- Keep back straight, shoulders relaxed, screen at eye level
- Use lumbar support (rolled towel or lumbar roll)
- Hips back in chair, feet flat on floor or footrest
- Knees at or below hip level
- Sit with slight recline (105-110°)
- Change position every 20-30 minutes
- Take brief walking breaks every 45-60 minutes during travel
Read More:
Top Remedies to Relieve Lower Back Pain
Lower Back Spasms That Prevent Movement
Conditions That Affect L4 and L5 Vertebrae
Ergonomic Tools That Actually Help
You don’t need a showroom makeover. Start with targeted supports and scale up if needed.
- Lumbar roll or pillow: Inexpensive, high-impact for desk and car.
- Ergonomic chair: Adjustable lumbar, seat height/depth, and recline. Waterfall front edge helps if you feel hamstring tension.
- Footrest: Essential if your feet don’t comfortably reach the floor.
- Adjustable bed or wedges: For those who prefer reclined sleep without aggravating the low back.
- Knee pillow: Keeps pelvis neutral for side and back sleeping.
- Short-term back brace: May help during flares or specific tasks; use under clinician guidance to avoid deconditioning.
Lifestyle Strategies: Build a Back-Friendly Routine
The best results usually come from “a little, often” rather than “a lot, rarely.”

- Activity first: Daily walking (10-20 minutes) or gentle cycling improves blood flow and eases stiffness.
- Core endurance over crunches: Think bracing, dead bug, bird-dog, and side planks – movements that build support without hyperextension.
- Hips matter: Glute bridges, clamshells, and hip flexor stretches reduce compensations at the lumbar spine.
- Flexibility: Hamstring, hip flexor, and piriformis stretches support neutral alignment.
- Flare management: Heat for muscle guarding; cold for sharp, inflamed pain.
- Sleep + stress: Consistent bedtimes and wind-down routines can lower pain sensitivity and speed recovery.
When to Consider Surgery

Most people improve with conservative care within weeks to months. Consider surgical consultation if:
- Pain or neurological symptoms persist despite comprehensive non-surgical care.
- There’s significant or progressive weakness, numbness, or changes in bowel/bladder function.
- Imaging shows high-grade slip or instability correlating with your symptoms.
Common procedures:

- Decompression: Removes pressure from nerves when stenosis dominates your symptoms.
- Fusion: Stabilizes the slipped level but limits motion.
- Motion-preserving alternatives: The TOPS System is designed to stabilize while preserving segmental motion. It may be appropriate for select patients – ask a spine specialist if you’re a candidate.
David danced at his son's wedding Bonnie explains why TOPS surgery was the right decision for her Wade is back to hiking Scott speaks about going to surgeryPremia Spine TOS System Testimonials




What Worsens Spondylolisthesis?
High-impact exercise, poor posture, excessively twisting the spine, and prolonged bed rest can worsen spondylolisthesis.

High-impact exercises like running, jumping, weightlifting, and contact sports can worsen spondylolisthesis. These activities place excessive impact on the spine, which can exacerbate back and nerve pain. They also create the risk of acute injuries, like fractures and contusions, which can lead to more pain.
- Poor posture can worsen spondylolisthesis. When the spine isn’t in proper alignment, it strains the spinal structures and can aggravate nerve impingement from spondylolisthesis.
- Excessive spinal twisting with spondylolisthesis can lead to worsened back pain and nerve impingement. Certain activities like gymnastics, diving, tennis, and golf require deep spinal twists. So, it’s best to avoid these if you’ve been diagnosed with spondylolisthesis.
- Prolonged bed rest may seem like a good way to take stress off the spine. However, this is a common mistake. While your doctor may recommend some rest after your spondylolisthesis diagnosis, don’t stay in bed for extended periods.
- Bed rest can cause muscle tension, which can worsen your symptoms. Over time, it may also cause muscle atrophy. If the muscles that support the spine weaken, it will increase the impact on your spine with day-to-day movements.
What About Asymptomatic Spondylolisthesis?
It’s also worth noting that some cases of spondylolisthesis are asymptomatic. This occurs if the vertebra slips out of place, but doesn’t irritate nearby spinal nerves. If you have asymptomatic spondylolisthesis, you can often safely perform any activity that doesn’t trigger pain or neurological symptoms.
Summary:
- High-impact exercise (running, jumping, weightlifting, contact sports) increases spinal impact, can exacerbate back and nerve pain, and raises the risk of acute injuries (fractures, contusions).
- Poor posture strains spinal structures and can aggravate nerve impingement when the spine is out of alignment.
- Excessive spinal twisting (e.g., gymnastics, diving, tennis, golf) can worsen back pain and nerve impingement; best avoided after diagnosis.
- Prolonged bed rest is a common mistake: it can cause muscle tension and, over time, muscle atrophy. Weak support muscles increase spinal load during daily activities.
Read More:
What Makes Spondylolisthesis Worse?
Critical Signs Your Lower Back Pain Is a Medical Emergency
Lower Back and Hip Pain: Common Causes and Solutions
Regain your mobility with Premia Spine! Contact us now
FAQ: Quick Answers
- Best sleeping position?
- Back with a pillow under your knees or a gentle recline. Side sleeping with a knee pillow works for many.
- Can sitting worsen it?
- Prolonged slouched sitting can. Use lumbar support, a slight recline, and frequent movement.
- Best chair?
- Adjustable lumbar support, seat height/depth, and 105-110° recline.
- Is walking good?
- Yes, low-impact movement is often well-tolerated and helpful.
- Stomach sleeping
- Usually not ideal; if you must, place a pillow under your hips.
- How long to improve?
- Many feel better within weeks with consistent positioning and exercise.
- Car Seat Support Tips?
- Use a lumbar roll in your car to support the natural curve of your lower back during drives.
- How Long Sit Safely?
- Limit sitting to 30-45 minutes at a time, then stand or walk briefly to relieve spinal pressure.
- Getting Into Bed?
- Sit on the edge of the bed, swing legs up together, then use arms to lower yourself smoothly-avoid twisting.
- Best Sitting Posture?
- Sit with back supported, feet flat, knees level with hips.
- Driving with Spondylolisthesis?
- Yes, use lumbar support and take hourly stretch breaks.
- Back Sleeping Okay?
- Yes, with a pillow under the knees to support the neutral spine.
- Mattress Firmness?
- Choose medium-firm for spinal alignment and pressure relief.
- Back Brace at Night?
- Not recommended; may restrict movement and reduce comfort.