



Common Problems After Spinal Fusion: Short-Term Risks vs. Long-Term Complications
While spinal fusion effectively stabilizes the spine, its recovery process is often complex. Patients may face two types of problems: symptoms that appear early in the post-op stage, or long-term concerns like adjacent segment disease (ASD) and hardware failure.
Common Issues at a Glance
| Timeline | Common Problems | Risk Level |
| 1 to 6 Weeks | Muscle stiffness & weakness, nerve symptoms, incision site pain, fatigue, constipation | Common, to be expected |
| 3 to 12 Months | Pseudoarthrosis (failed fusion), screw loosening, persistent pain, scar tissue formation | Pseudoarthrosis: 5 to 15%Screw loosening: 1 to 60%Persistent pain: 8 to 40%Scar tissue: Common, to be expected |
| 2 to 10 Years and Beyond | Adjacent segment disease (ASD), reduced mobility | ASD: ~11.7%Reduced mobility: Relatively common |

Let’s break down the possible complications at every stage of the spinal fusion recovery process, from normal post-op pain to failed fusion, and learn about motion-preserving alternatives that can help you avoid these common problems.
Immediate Post-Op Red Flags: When to Seek Emergency Care
Infection, blood clots, nerve damage, and cauda equina syndrome are possible fusion complications that require immediate medical attention. Go to the emergency room if you experience any of these red flag symptoms:
- Infection
- Pain around the incision (usually around one month post-op)
- Redness, swelling, and warmth around the incision
- Fever or chills
- Foul-smelling discharge or pus from the incision
- Blood clots (deep vein thrombosis)
- Pain, throbbing, swelling, redness, and warmth in one leg (rarely both legs)
- Nerve damage
- Bowel or bladder dysfunction
- Sexual dysfunction
- New or worsening nerve symptoms, like tingling, numbness, and weakness
- Difficulty walking, balancing, or lifting your legs
- Cauda equina syndrome
- Bowel or bladder dysfunction
- Sexual dysfunction
- Saddle anesthesia (numbness in the inner thighs, buttocks, and perineum)
Can Spinal Fusion Cause Paralysis?
Spinal fusion can cause paralysis, but it’s one of the rarest possible complications. New major neurological deficits occur in less than 0.2% of spinal surgeries. When it does happen, paralysis may stem from one of the following problems during the procedure:
- Extradural spinal hematoma, which involves bleeding within the spinal column
- Incidental durotomy, which occurs when spinal fluid leaks
- Accidental injury to the nerves when they’re repositioned during the operation
- Accidental injury to the blood vessels that deliver blood to the spinal cord
Complications at 3 to 12 Months: Pseudoarthrosis, Screw Loosening, Nerve Irritation
At the 3-to 12-month mark, fusion complications may include pseudoarthrosis, screw loosening, scar tissue, or nerve irritation.
- Failed fusion (pseudoarthrosis) occurs when the targeted vertebrae fail to fuse properly.
- Symptoms: Chronic back pain, radiculopathy, neuropathic pain, reduced mobility
- Incidence: 5% to 15%, according to a BMC Musculoskeletal Disorders study
- Screw loosening after fusion can result from poor bone quality (usually from osteoporosis), fusion failure, or not adhering to the “BLT” restrictions (no bending, lifting, or twisting).
- Symptoms: Recurring pain, stiffness, nerve irritation, crepitus (grating or popping sensation in the affected part of the spine)
- Incidence: ~15% in people with normal bone density, up to 50% in people with osteoporosis, according to a World Neurosurgery study
- Epidural fibrosis: Scar tissue formation is inevitable after surgery. But when it forms excessively around the nerve roots in the spine, it’s called epidural fibrosis. Scar tissue has been found to cause 20% to 30% of failed back surgery syndrome (FBSS) cases.
- Symptoms: Pain, radiculopathy, reduced mobility
- Incidence: Some degree of scar tissue forms in 24% to 100% of back surgery patients; over 83% of patients with persistent pain after back surgery had severe epidural fibrosis.
- Nerve irritation caused by nerve disruption during surgery, scar tissue, inadequate decompression, or altered spinal mechanics can trigger symptoms after fusion. It may heal on its own or, less commonly, require further treatment.
- Symptoms: Radiating pain, burning pain, numbness, tingling, weakness
- Incidence: Temporary nerve damage is common during the recovery phase; new permanent nerve damage occurs in less than 1% of cases.
Is Persistent Nerve Pain Normal 6 Months After Spinal Fusion?
It’s generally considered “normal” to experience fluctuating pain levels and nerve sensations in the first 6 months after spinal fusion, and it can take a year for nerves to fully heal after surgery. However, you should call your doctor if you experience:
- Sudden, severe, new, or worsening numbness, tingling, weakness, or radiating pain
- Bowel, bladder, or sexual dysfunction
- Nerve pain that doesn’t improve with your prescribed pain relief methods (medications, PT, home care, etc.)
Long-Term Complications: Life After Spinal Fusion
Possible long-term problems after spinal fusion include adjacent segment disease (ASD), failed back surgery syndrome (FBSS), chronic pain, and mobility limitations.
- Adjacent segment disease occurs when the fused spinal segment alters load-bearing across the spine, forcing other spinal levels to absorb more impact and degenerate more rapidly than usual.
- Symptoms: Back pain, radiculopathy (tingling, numbness, weakness), stiffness
- Incidence: An estimated 11.5% (after instrumented fusion in adults with lumbar spondylolisthesis, according to a Clinical Neurology and Neurosurgery study)
- Failed back surgery syndrome (FBSS) is the general term for new back or leg pain after spinal surgery. The pain may start after surgery, or the procedure may fail to meaningfully improve the patient’s condition.
- Symptoms: Chronic or recurring back or leg pain that doesn’t improve during the healing process, neurological symptoms, reduced mobility
- Incidence: 10% to 40%, according to a Journal of Pain Research study
Psychological Concerns Following Spinal Fusion
Psychological distress is a prevalent issue among people with continued back and leg symptoms after spinal fusion. Psychological factors like catastrophizing and fear-avoidance can also negatively impact post-fusion recovery. A Spine study reported a 6% rate of new-onset depression and an 11.2% rate of new-onset anxiety after spinal fusion.
These strategies can mitigate the psychological impact of spinal fusion:
- Setting realistic expectations
- Solidifying a strong support system, including professional mental health support as needed
- Committing to physical therapy and a gentle exercise plan
- Managing stress and prioritizing sleep
- Spending time outdoors, journaling, meditating, and engaging in social activities

Risk Factors for Fusion Complications
Nicotine use, obesity, mechanical stress, and underlying medical conditions like osteoporosis and diabetes are risk factors for fusion complications.
- Nicotine use: Smoking, vaping, or using other nicotine products raises your risk for pseudoarthrosis because it constricts blood vessels, which impairs osteoblast function and increases bone resorption. An Advanced Spine Journal study found that 33.33% of smokers experienced incomplete or no fusion (compared to 6.12% of non-smokers).
- Osteoporosis, a bone disease characterized by weak, brittle bones, increases the risk of pseudoarthrosis, hardware failure, and revision surgery. A Global Spine Journal study found that 50% of patients with osteoporosis who underwent lumbar fusion experienced osteoporosis-related complications (revision surgery, compression fracture, proximal junctional kyphosis, pseudoarthrosis, or failed instrumentation).
- Diabetes significantly raises the risk of failed lumbar fusion requiring revision surgery, according to a JBMR Plus study. This condition also predisposes the adjacent spinal segments to degeneration, likely due to poor circulation and diminished bone healing.
- Obesity has been linked to high nonunion rates, worse patient outcomes, and a higher risk of post-op complications, including infections, prolonged wound healing, and instrumentation failure, according to a Spine study.
- Mechanical stress from the BLTs (bending, lifting, twisting), repetitive movements, and high-impact activities can lead to fusion complications.
Spinal Fusion Recovery and Outlook: From the Hospital to One Year Post-Op
Full recovery following spinal fusion typically takes six to 12 months in total, with a relatively positive outlook for patients who follow all aftercare instructions and maintain a healthy lifestyle.
During spinal fusion recovery, you can expect to gradually return to your normal activities. While this timeline varies significantly based on age, overall health, and the number of fused levels, here’s a general estimate:
- After three to four days, most patients return to the hospital.
- After two to four weeks, most patients can engage in gentle movements and start seeing a physical therapist.
- After four to six weeks, most patients can engage in some low-impact exercise, and those with non-physically demanding jobs can return to work.
- After three to six months, most patients increase their activity levels, and those with mildly physically demanding jobs can return to work.
- After six to 12 months, most patients make a full recovery and return to all of their normal activities, except for certain high-impact exercises and extreme spinal twisting or bending.
Mitigating Post-Op Risks and Fusion Alternatives
To mitigate risks and prevent post-surgical complications after spinal fusion, it’s important to follow all of your surgeon’s aftercare instructions, attend all recommended follow-up appointments, care for your wound properly, and maintain a healthy lifestyle.
- Your surgeon’s aftercare instructions help prevent complications and help your body heal as effectively as possible. They may include activity restrictions, medication prescriptions, and certain lifestyle recommendations, like quitting smoking, avoiding alcohol, and eating an anti-inflammatory diet.
- Ongoing follow-up appointments allow your surgeon to monitor your recovery progress and catch early signs of complications, before they become severe. They also allow your surgeon to provide personalized guidance about when to return to work and physical activity. Attend all of these appointments as advised, as well as all recommended physical therapy appointments, to rebuild strength and mobility.
- Proper wound care typically involves keeping the wound dry for the first few days and monitoring it for warning signs, like extra fluid drainage, warmth, and worsening redness or swelling.
- Maintaining a healthy lifestyle helps prevent post-surgical complications by ensuring your body has the tools it needs to heal. This means engaging in gentle movement (as advised by your doctor), quitting smoking, limiting alcohol consumption, and eating a balanced, nutritious diet.
What Helps Nerve Pain in the Legs After Back Surgery?
Pain medications, physical therapy, exercise, cold therapy, and spinal cord stimulation can help nerve pain in the legs after back surgery.
- Pain medications like NSAIDs and acetaminophen can alleviate pain in the legs while the nerves heal.
- Physical therapy supports the nerve healing process and prevents further irritation. Your PT may recommend dynamic lumbar stabilization exercises, which specifically target the muscles that support the spine. When these muscles are stronger, they can protect the spinal nerves from impact.
- Exercise: While some bed rest after surgery is essential, prolonged periods of it should be avoided. Low-impact exercise, like walking and swimming, can alleviate inflammation, improve muscle strength, and boost circulation to the healing nerves.
- Cold therapy is a simple way to reduce inflammation in the areas affected by post-operative nerve pain. You can use an ice pack at home, or consider more advanced cryotherapy methods from local providers.
- Spinal cord stimulation administers gentle electrical impulses to certain nerves in the spinal cord. This process may intercept pain signals before they’re delivered to the brain, providing pain relief. Spinal cord stimulation is widely used to treat failed back surgery syndrome.

A Motion-Preserving Alternative to Prevent ASD
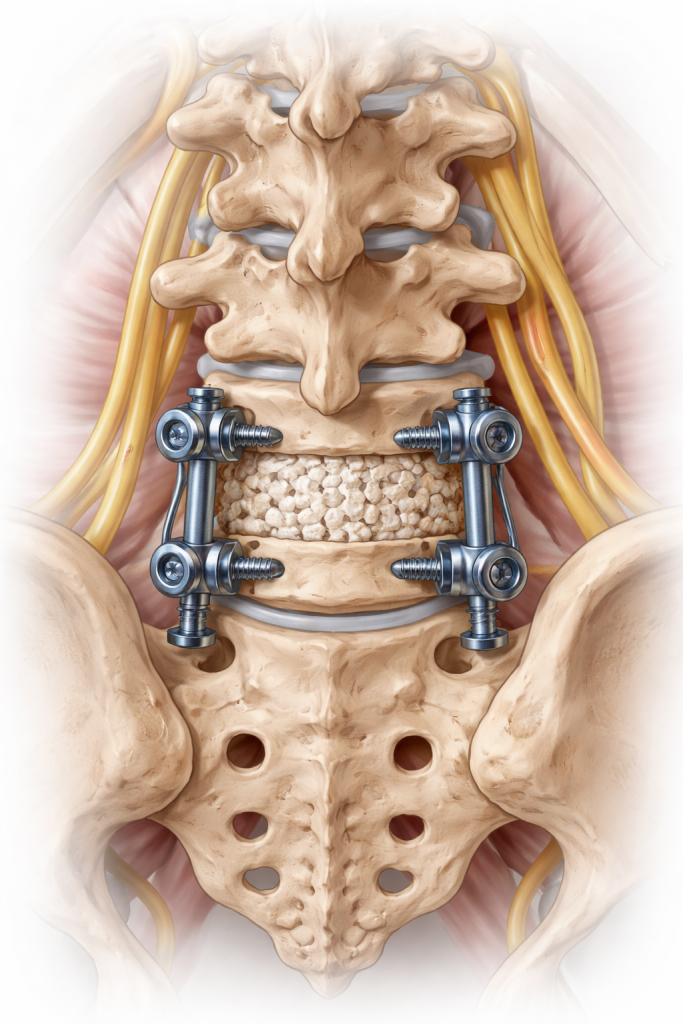
The TOPS System is an FDA-approved, motion-preserving implant that stabilizes the spine without fusing the vertebrae. It’s earned a superior-to-fusion claim from the FDA, and the device moves with the spine to create a controlled range of motion.

The TOPS System works by replacing the spinal structures removed during spinal decompression. It’s anchored to the spine and includes a patented crossbar configuration, which exerts less impact on the screws than fusion implant devices. The device recreates motion in every direction, including flexion, extension, axial rotation, and lateral bending.
David danced at his son’s wedding Bonnie explains why TOPS surgery was the right decision for her Wade is back to hiking Scott speaks about going to surgeryReturn to normal with Premia Spine!




Regain your mobility with Premia Spine! Contact us now
In a study of the TOPS System for lumbar spinal stenosis and degenerative spondylolisthesis, the visual analog scale (VAS) for back and leg pain lowered from 56.2 before the procedure to 12.5 at six weeks, 13.7 at one-year follow-up, 3.6 at two years follow-up, and 19 at seven years follow-up. These results showed that TOPS can continue to provide clinical improvement over time.
Patients who are concerned about the complications from spinal fusion can speak with a specialist in their area to learn more about the available alternatives.
FAQs
- How do I know if my spinal fusion failed?
- Warning signs of fusion failure include chronic pain at the fusion site, pain that radiates from the fusion site to the lower extremities, neurological symptoms (numbness, weakness, or tingling), and reduced mobility.
- How do I know if my hardware is loose after spinal fusion?
- Warning signs of loose hardware after fusion include recurring pain at the surgical site, reduced mobility, neurological symptoms, and crepitus (grinding, clicking, or popping) at the fusion site.
- What are the symptoms of a broken screw in the spine?
- Worsened or returning pain, radiculopathy, numbness, tingling, weakness, and reduced mobility
- How long does it take for nerves to heal after fusion?
- Up to two years
- Is nerve pain normal one year after fusion?
- Significant nerve pain isn’t normal one year after fusion and merits an appointment with your doctor.